
Here’s a situation almost every Indian in their 20s or 30s will recognise: the pimple is gone, but the face still looks like something happened. Maybe it’s a flat dark patch. Maybe it’s a red or pink mark. Maybe it’s a small pit or indent in the skin. You try brightening serums, spot treatments and SPF religiously — and a year later, some of those marks are still there while others have faded. What’s going on?
The answer almost always comes down to one misunderstood distinction: the difference between acne marks and acne scars. They look similar to the untrained eye. They feel similar when you run your fingers across them. But they are completely different things, at completely different levels of the skin — and the treatments that fix one do almost nothing for the other. This is the most common reason people spend months on the wrong treatment and feel like their skin isn’t improving.

Here’s the clear guide nobody gave you.
| TL;DR — the 60-second version
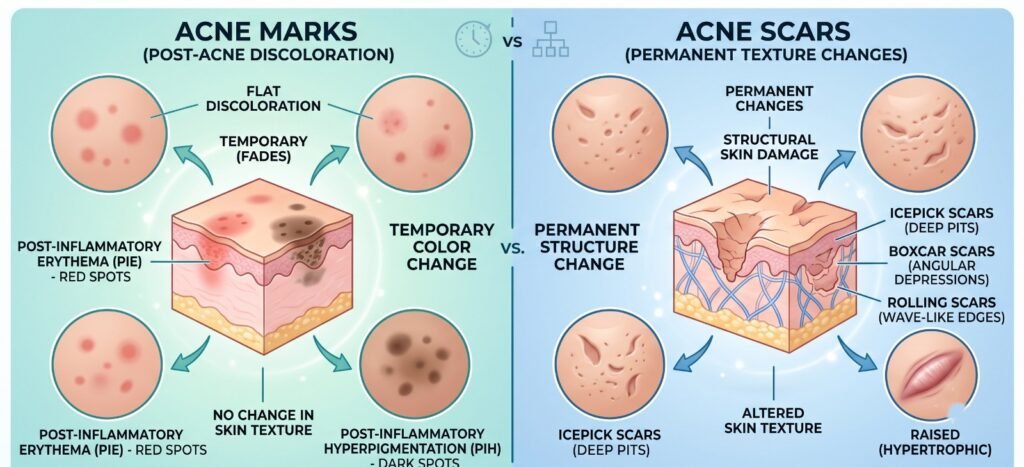
Acne MARKS are changes in colour left after a pimple heals — flat, no texture change, they will fade on their own (faster with the right treatment). Three types: PIH (dark/brown marks, very common in Indian skin), PIE (red/pink marks from dilated blood vessels), and post-acne erythema. Acne SCARS are changes in TEXTURE and STRUCTURE — pits, indents, raised tissue — caused by permanent damage to the dermis. They do NOT fade on their own and need professional treatment. Most people with post-acne skin have BOTH, which is why a proper skin assessment before starting treatment is essential. The wrong treatment wastes time and money. |
The Four Things in Acne Marks vs Acne Scars You Might Be Looking At
Before diving into treatment, you need to identify which of these four things you actually have. This is the diagnosis that drives everything else:
| What you see | What it is | Level of skin affected | Does it fade on its own? |
| Flat dark brown / grey patch where a pimple was | Post-inflammatory hyperpigmentation (PIH) | Epidermis (surface) | Yes, slowly — months to years without treatment |
| Flat red or pink mark where a pimple was | Post-inflammatory erythema (PIE) | Upper dermis (dilated capillaries) | Yes, slowly — faster with targeted treatment |
| A small pit, indent, or depression in the skin | Atrophic acne scar (ice pick, boxcar, rolling) | Dermis — permanent structural damage | No. Needs professional treatment. |
| A raised, firm lump or thickened skin where a pimple was | Hypertrophic scar or keloid | Dermis — excess collagen deposition | Rarely. Needs professional treatment. |
The Simple Test: Acne Marks vs Acne Scars in Under 30 Seconds
You don’t need a doctor to do this initial check — though you do need one to plan treatment.
- Look at your skin in good lighting (natural daylight, not bathroom mirror lighting).
- Run your clean fingertip gently over the area that concerns you.
- Ask yourself: is the surface flat and smooth under your finger, or does it feel uneven, indented or raised?
Flat and smooth under the finger = a mark (PIH or PIE). Colour change only, no texture change.
Uneven, indented or raised = a scar. Structural change in the skin.
If you can feel a change in surface texture, that’s a scar and it needs professional treatment — no skincare product will fix a structural change in the dermis. If the skin surface is smooth and you’re only looking at colour, that’s a mark — treatable with skincare and accelerated with clinical treatment.
| Why this matters so much for Indian skin specifically
Indian skin (Fitzpatrick types IV and V) is significantly more prone to post-inflammatory hyperpigmentation than lighter skin types. When the skin is inflamed — by a pimple, a scratch, an abrasion, even an aggressive skincare product — the melanocytes (pigment-producing cells) over-respond and produce excess melanin. This is PIH. It’s not a scar, it’s a pigment response. But because it looks so persistent and dark in Indian skin, it’s routinely mistaken for scarring — and treated with scar protocols that won’t touch it. Meanwhile, the PIH quietly fades on its own while patients conclude the treatment ‘worked.’ The real risk: treating PIH aggressively with the wrong approach (like certain lasers or harsh exfoliants) can actually create more PIH. |
Acne Marks: What They Are and How to Treat Them
PIH — Post-Inflammatory Hyperpigmentation (Dark Marks)
PIH is not a scar. It’s a pigment response: when the skin is inflamed, melanocytes produce excess melanin as a protective reaction, and that melanin sits in the epidermis (and sometimes the upper dermis) as a flat, dark patch. It always fades eventually — but ‘eventually’ without intervention can be 12–24 months or longer in Indian skin, and sun exposure keeps resetting the clock.
What actually helps PIH:
- Sunscreen (SPF 50+) every morning, non-negotiable. UV exposure darkens existing PIH and prevents new marks from fading. This single step makes more difference than any treatment you’ll pay for.
- Topical actives: niacinamide (reduces melanin transfer), azelaic acid, tranexamic acid, vitamin C, kojic acid, alpha arbutin. These work slowly and need 8–12 weeks of consistent use.
- Chemical peels: glycolic and lactic acid peels accelerate cell turnover, bringing fresh skin to the surface faster. Mandelic acid peels are a good first choice for Indian skin (gentle and less likely to trigger more PIH).
Hollywood Spectra / Q-switched laser toning: targets excess melanin directly without ablating the epidermis. A strong clinical option for stubborn PIH that’s not responding to topicals.
- Mesotherapy and skin boosters: cocktails with glutathione, tranexamic acid and vitamin C delivered directly into the skin brighten PIH faster than topical application alone.
PIE — Post-Inflammatory Erythema (Red / Pink Marks)
PIE is a different problem. Those red or pink marks are from dilated capillaries in the upper dermis left over from the inflammation of a pimple. The blood vessel walls were damaged by the acne inflammatory process and haven’t fully recovered. PIE is more common in lighter skin tones but absolutely occurs in Indian patients too, and is often mistaken for ongoing active acne or for PIH.
PIE needs different treatment from PIH:
- SPF protection to prevent worsening (same as PIH)
- Pulsed dye laser or vascular laser: directly targets dilated blood vessels
- Niacinamide in topicals: reduces redness and inflammation
- Azelaic acid: anti-inflammatory, works on both PIH and PIE
- Time: PIE often fades on its own, just more slowly than PIH
Acne Scars: What They Are and Why They Need Professional Treatment
Acne scars are what happen when the inflammation from a pimple damages the dermis — the deeper, structural layer of skin below the epidermis. Unlike marks, this damage is permanent. The body tries to repair it with collagen, but the repair is imperfect: sometimes too little collagen is produced (leaving a pit or indent), sometimes too much (leaving a raised bump).
Atrophic scars (the depressed/pitted type) — most common
- Ice pick scars — deep, narrow, V-shaped pits that look like the skin was punctured with a sharp instrument. Most common on cheeks.
- Boxcar scars — wider, round depressions with defined vertical edges. Like small craters.
- Rolling scars — broad, shallow depressions with sloping edges, giving the skin a wavy or undulating appearance.
Hypertrophic and keloid scars (the raised type)
- Hypertrophic scars — raised, firm scars that stay within the boundary of the original pimple. More common on the back, chest and jawline.
- Keloids — raised scars that grow beyond the original boundary, sometimes itchy. More common in darker skin types; needs careful management.
| Why acne scars don’t go away on their own
PIH and PIE fade because the pigment metabolises and the blood vessels normalise — slow, but it happens. Atrophic scars don’t fade because the dermis was physically destroyed and incompletely repaired. No skincare product can reach into the dermis to rebuild collagen structure. That’s not marketing; it’s anatomy. The treatments that work for scars — RF microneedling, subcision, TCA CROSS, fractional laser — all work by creating a new, controlled injury deeper in the skin that triggers a proper collagen repair response. |
Treating Acne Scars: The Tools That Actually Work
The right scar treatment depends on the scar type — ice picks need different tools than rolling scars. Our full acne scar treatment guide covers the complete range. A quick summary:
- Rolling scars — subcision (releasing the tethered fibrous bands pulling the skin down) + filler or PRP. The gold standard.
- Ice pick scars — TCA CROSS (applying high-strength TCA into each individual scar). Targeted and precise.
- Boxcar scars — fractional CO2 laser, RF microneedling, or punch elevation for sharp-edged individual scars.
RF microneedling (Morpheus8) and MNRF: rebuild collagen across the whole treated area, improving multiple scar types simultaneously. Particularly well-suited to Indian skin.
Dermapen 4 microneedling with PRP: a strong, accessible option for broad atrophic scarring; the PRP accelerates the collagen response.
Fractional CO2 laser: one of the most powerful resurfacing options, best reserved for significant scarring; requires careful settings in Indian skin.
The Part Nobody Tells You: Most People Have Both
Here’s the honest reality of what a typical post-acne face looks like at 25: some rolling scars on the cheeks, a couple of ice picks at the side, and a layer of PIH and PIE all over — which makes the scars look even worse by adding colour on top of the texture change.
A good treatment plan doesn’t just pick one. It:
- Addresses the active acne first (if still breaking out — no point treating scars when new ones keep forming)
- Targets the PIH in parallel with brightening treatment and pigment lasers
- Treats the scars with the right technique for each scar type
- Sequences them correctly — deep scar work on a face still covered in PIH risks additional pigmentation around the treated areas
This is why ‘I tried microneedling and it didn’t help my marks’ is such a common complaint — because microneedling is primarily a scar treatment, not a pigment treatment. And ‘I used brightening serum for a year but my pits are still there’ is equally common — because serums address pigment, not dermal structure. The sequencing and targeting of the right treatment for the right problem is what acne scar treatment at a proper clinic actually looks like.
A Note on Indian Skin: Why Aggressive Treatment Often Backfires
This section deserves its own space because it’s genuinely different for Indian skin and most generic skincare advice doesn’t account for it.
Fitzpatrick IV-V skin has a higher density of active melanocytes, which means it responds to inflammation by producing more pigment. This includes the inflammation caused by acne treatment itself. The common mistake: using a treatment that’s too aggressive for the scar (e.g. high-energy ablative laser) and creating a ring of PIH around the treated scar that looks worse than the original problem.
The guiding principles for Indian post-acne skin:
- SPF 50+ every morning, no exceptions. Sun exposure doubles the time PIH takes to fade and worsens hyperpigmentation after any clinical treatment.
- Start lower and build. Begin with gentler treatments (mandelic peels, microneedling) and escalate to stronger options (fractional CO2) only if needed and with a proper patch test.
- Control active acne first. Every new pimple risks more PIH. Anti-acne treatment first is an investment in scar and pigment treatment later.
- Address the PIH and scars together, in the right order. Don’t try to do both at maximum settings simultaneously; sequence the treatments properly.
For the full Indian-skin approach to acne treatment and open pores management that comes alongside acne, both are covered in detail on their respective pages.
Frequently Asked Questions
How can I tell the difference between acne marks and acne scars?
Run a clean fingertip over the skin in good lighting. If the surface is flat and smooth and only the colour is different (dark, red or pink patch), it’s a mark (PIH or PIE). If you can feel an indent, pit or raised area, it’s a scar. This takes 30 seconds and is the most important thing you can do before choosing any treatment.
Do acne marks go away on their own?
Yes, eventually — PIH (dark marks) typically fades over 6–24 months in Indian skin, faster with SPF and brightening actives, faster still with clinical treatment. PIE (red/pink marks) also fades on its own over months. Acne scars (textural changes like pits) do not fade on their own and need professional treatment.
What is the fastest treatment for acne marks in India?
SPF 50+ every morning is the single most important step and accelerates fading more than any other change. Clinically, Q-switched laser toning (Hollywood Spectra), chemical peels (mandelic or glycolic) and mesotherapy with brightening actives are the fastest ways to accelerate PIH fading. Results are usually visible in 4–6 weeks with consistent treatment.
Can serums and creams fix acne scars?
No — at least not the textural ones (pits and indents). Serums and creams address the epidermis and can significantly improve PIH and PIE, but they cannot reach into the dermis to rebuild the collagen structure destroyed by acne. For actual scars, you need professional treatments like RF microneedling, subcision, TCA CROSS or fractional laser.
Why does Indian skin get more dark marks after acne?
Indian Fitzpatrick IV-V skin has a higher density of active melanocytes (pigment-producing cells) that over-respond to inflammation. When skin is inflamed — by a pimple, a scratch or even an aggressive skincare product — the melanocytes produce excess melanin as a protective response, leaving behind a dark mark (PIH). This is completely normal physiology, not a sign of permanent damage.
Is RF microneedling (Morpheus8) good for acne marks or scars?
Morpheus8 and MNRF are primarily scar treatments — they rebuild collagen in the dermis to improve the texture of atrophic (pitted) scars. They have some secondary brightening effect through collagen turnover, but they’re not the primary treatment for PIH (dark marks). For PIH, pigment-targeting treatments like Q-switched laser toning and brightening peels work better.
What happens if I treat acne marks with a scar treatment?
The treatment usually doesn’t help the marks (because it’s targeting the wrong layer of skin), and in darker skin tones it can actually worsen PIH by causing additional inflammation in the epidermis. This is the most common reason patients feel like ‘nothing works’ — they’ve been using scar treatments for marks, or brightening treatments for scars.
Should I treat acne marks or scars first?
Usually active acne first (stop making new ones), then marks and scars together but in the right sequence — stabilise the PIH with SPF and brightening treatment first, then layer in scar-specific treatment (microneedling, subcision, laser) once the pigment is more stable. Aggressive scar treatment on skin still covered in active PIH can worsen the pigmentation around the treated area.
The difference between an acne mark and an acne scar is the difference between a colour change and a structural change. One lives in the epidermis and fades. The other lives in the dermis and stays until it’s specifically treated. Most people with post-acne skin have both — which is exactly why a proper skin assessment before starting any protocol matters so much.
If you’re unsure which you’re dealing with, or if you’ve been treating your skin for months without seeing the right results, a consultation is the most efficient next step. Book with Dr. Adarsh Tripathi at Sarayu Clinics, Greater Kailash — book online here or call +91 9289111081.



{kind=link}
{kind=link}