Wart Removal in Delhi
Wart Removal in Delhi
Warts are an infection, not a blemish. That single fact — obvious once said, and rarely said — explains almost everything patients find frustrating about them. It explains why they come back after being burned off. It explains why one appears and then three more follow. It explains why a treatment that worked perfectly for your colleague did nothing for you. And it explains why the most important question is not which laser, but what is your immune system doing about the virus.
A wart is a lump of skin cells growing too fast because they have been infected by a human papillomavirus. Destroying the lump — with cold, with heat, with light, with a blade — removes what you can see. It does not remove the virus, which is also sitting quietly in the normal-looking skin around it. Any clinic promising permanent removal in a single session is describing the lump and ignoring the infection.
At Sarayu Clinics in Greater Kailash, warts are assessed and treated by facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi. This page will tell you what a wart actually is, how to know whether the thing on your foot is even one, which treatments make sense for which warts, why recurrence happens, when the honest answer is to do nothing at all — and the small number of cases where a lesion that looks like a wart is something that needs a biopsy.

The short answer : Warts are benign skin growths caused by human papillomavirus (HPV) infecting the outer layer of skin. They are contagious, they spread by direct contact and by autoinoculation (scratching one and seeding another), and they enter through tiny breaks in the skin. Common types: common warts on hands and knees; plantar warts on the soles; flat warts on the face; filiform warts around the eyelids, lips and neck; periungual warts around the nails. No treatment eradicates HPV — every method destroys the visible wart while the virus may persist in surrounding skin, which is why recurrence is common and expected rather than a sign of failure. A substantial proportion of warts clear on their own within one to two years in people with healthy immune systems. Treatments include topical salicylic acid (the best-evidenced and cheapest), cryotherapy, radiofrequency ablation, electrocautery, CO2 laser, and — for multiple or stubborn warts — intralesional immunotherapy, which uses your own immune system to clear even the warts that were never injected. Delhi cost: roughly Rs 500–2,000 per wart for cryotherapy, Rs 1,500–8,000 for laser or RF, Rs 1,500–4,000 per immunotherapy session. Surgical excision is rarely the right answer. A wart that will not respond to treatment needs a biopsy, not another session.
Is It Actually a Wart?
A surprising number of people who arrive asking for wart removal do not have a wart. The commonest confusions are worth thirty seconds of your time, because they lead to completely different treatments.
Wart, corn or callus? The test
This matters most on the sole of the foot, where a plantar wart and a corn feel identical to the person standing on them.
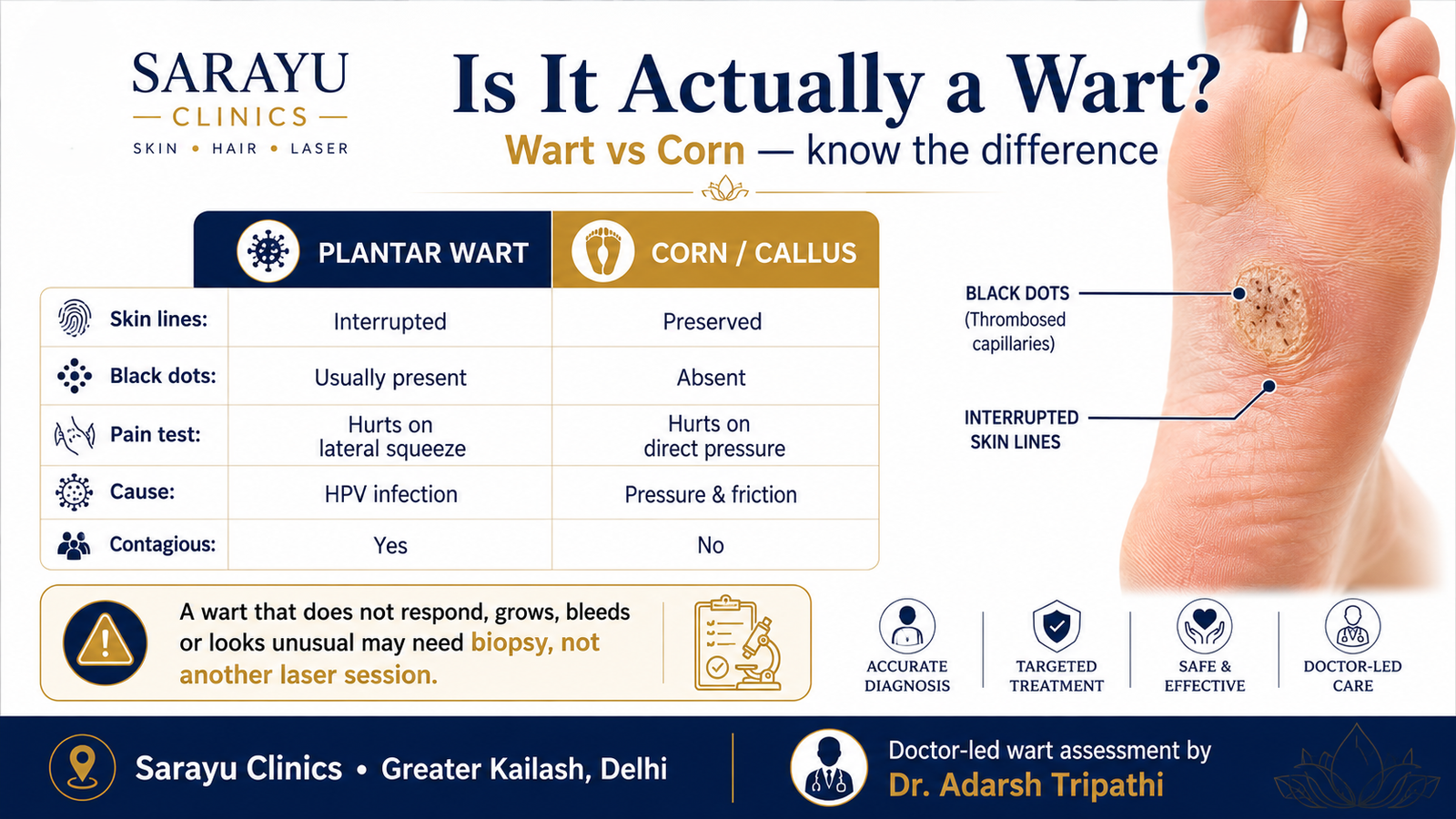
Feature | Plantar wart | Corn or callus |
Skin lines (the fine ridges of your fingerprint or sole) | Interrupted — the lines stop at the lesion and go around it | Preserved — the lines run straight across the lesion |
Tiny black dots | Usually present — these are thrombosed capillaries, not ‘seeds’ or ‘roots’ | Absent |
Pain on squeezing the lesion from the sides | Painful | Not particularly |
Pain on pressing directly down on it | Less painful | Painful |
Cause | HPV infection | Pressure and friction |
Contagious | Yes | No |
The black dots are the giveaway, and they are widely misunderstood. Patients are told they are the wart’s ‘roots’ or ‘seeds’ and that these must be dug out. They are neither. They are small blood vessels that have clotted inside the wart. Warts have no roots. Nothing needs to be dug out, and digging is how scars are made.
Other things that are not warts
Seborrhoeic keratoses — waxy, ‘stuck-on’ brown patches — are frequently mistaken for warts. They are entirely benign, not viral, and not contagious. Dermatosis papulosa nigra, the small dark papules common on the cheeks in darker skin, is likewise not a wart. Skin tags are not warts. Molluscum contagiosum is a different virus and behaves differently. All of these are treatable, several of them at this clinic, but the treatment differs — see our mole and lesion removal page.
The one that matters: when a wart is not benign : Squamous cell carcinoma, verrucous carcinoma and — rarely but importantly — amelanotic melanoma can all present as a rough, raised, wart-like lesion that does not respond to treatment. This is uncommon. It is also the reason we assess before we ablate. // The features that should prompt a biopsy rather than another session: a ‘wart’ that has failed two or more appropriate treatments; one that is growing steadily; one that bleeds without being knocked; one that has become painful or ulcerated; a solitary lesion appearing for the first time in an adult over 50; any warty lesion in someone who is immunosuppressed. // Cryotherapy, laser and radiofrequency all destroy the tissue, which means no specimen can be sent for histopathology. If a lesion is atypical or has not responded, the correct next step is to remove it in a way that preserves the tissue and send it to a laboratory. That is a surgical decision, and it is made before the machine is switched on, not afterwards.
The Types of Wart, and Where They Turn Up
Type | Where | What it looks like | Notes |
Common wart (verruca vulgaris) | Hands, fingers, knees, elbows | Rough, raised, cauliflower-like surface | The classic. Often self-resolves. |
Plantar wart (verruca plantaris) | Soles of the feet | Flat, pressed inward by body weight; black dots; painful | Deep and stubborn because pressure drives them inward. |
Flat wart (verruca plana) | Face, forehead, arms, shins | Small, smooth, barely raised; often many at once | Common in children and after shaving. Treat gently on the face. |
Filiform wart | Eyelids, lips, nose, neck | Thread-like, finger-shaped projections | Cosmetically prominent. Sits where scarring matters most. |
Periungual wart | Around and under fingernails and toenails | Rough, thickened, may distort the nail | Difficult. Nail-biting and cuticle-picking drive them. |
Mosaic wart | Soles, sometimes palms | A plaque of many small warts fused together | Notoriously resistant. Immunotherapy is often the answer. |
Anogenital wart (condyloma) | Genital and anal skin | Soft, flesh-coloured, sometimes clustered | A sexually transmitted infection. See the section below. |
Why Warts Come Back ?
This is the question every patient asks second, after the price, and the one that is answered least honestly.
Every wart treatment in existence — cryotherapy, laser, radiofrequency, cautery, acid, surgery — destroys wart tissue. None of them destroys human papillomavirus. The virus lives inside skin cells, and it is present not only in the visible wart but in a margin of skin around it that looks entirely normal, feels entirely normal, and cannot be seen even under magnification. Remove the wart perfectly, and the virus is still there.
What clears the virus is your immune system. That is why warts vanish spontaneously in some people and persist for years in others; why they multiply during a period of illness or stress; why they are commoner and more stubborn in people who are immunosuppressed. Treatment removes the lesion and buys the immune system time. The immune system does the rest, or it does not.
- Recurrence is expected biology, not treatment failure. Single common warts removed by laser or radiofrequency recur relatively infrequently. Multiple warts, mosaic warts and plantar warts recur far more often, because the reservoir of infected surrounding skin is larger.
- Treating every visible wart at once matters. Leaving one behind leaves a source that reseeds the others.
- Autoinoculation is real. Scratching, picking, shaving over a wart, biting nails around a periungual wart — each of these transports virus to a new site. The number of warts a patient has is often a measure of how much they have touched them.
- This is why immunotherapy is interesting. It is the only approach that addresses the reservoir rather than the lump.
The Option Nobody Offers You: Doing Nothing
A significant proportion of common warts in people with healthy immune systems disappear on their own within one to two years, without any treatment at all. The immune system eventually recognises the infected cells and clears them. No clinic makes money from this fact, which may be why it is so seldom mentioned.
We mention it because for some patients it is genuinely the right advice. A single, small, painless common wart on the back of a child’s hand, which is not spreading and not bothering anybody, does not necessarily need liquid nitrogen. It may need six months and a conversation about not picking it.
Treatment becomes clearly worthwhile when the wart is painful, when it is spreading, when it is on the face or the genitals, when it interferes with function, when it has been present for more than two years, when you are immunosuppressed or diabetic, or — legitimately — when it simply bothers you enough that you would rather it were gone. That last reason is a perfectly good one. It is just not a medical one, and we will not pretend otherwise.
Every Treatment, and What Each Is Actually For
Ordered roughly from gentlest to most aggressive. The right choice depends on the type of wart, where it is, how many there are, and how much scarring you can accept in that location.
Topical salicylic acid — the best-evidenced and the least profitable
Daily application of a keratolytic acid, softening and gradually dissolving the wart over weeks. It has among the strongest evidence bases of any wart treatment in the medical literature, comparable in several comparisons to cryotherapy, and it costs a few hundred rupees. It requires patience — twelve weeks of daily application is normal — and it requires that you pare down the surface regularly. It is the correct first-line treatment for most common and plantar warts in a compliant adult, and it is the treatment least likely to be recommended to you by a clinic, for reasons that are commercial rather than clinical.
Cryotherapy — liquid nitrogen
Freezing the wart to around minus 196 degrees, which destroys the infected cells and, usefully, provokes a local inflammatory response that helps the immune system notice the virus. Applied by spray or cotton bud, in freeze-thaw cycles. Repeated every two to three weeks, typically for three to six sessions. Stings sharply, blisters afterwards, and works. Poorly suited to the eyelid margin and to darker skin on the face, where it can leave a pale patch.
Radiofrequency ablation and electrocautery
Heat, delivered by a fine electrode, vaporises the wart under local anaesthetic. Precise, bloodless, and immediate — the wart is gone when you leave. Excellent for filiform warts, single common warts and warts around the nail. Depth control is the whole skill: too shallow and it recurs, too deep and it scars. No specimen is preserved for biopsy.
CO2 laser
Precisely controlled ablation, layer by layer, with excellent haemostasis. Particularly useful for periungual warts, plantar warts and lesions in awkward anatomical corners. It is not more effective than radiofrequency for a straightforward wart, and it costs more. As with RF, the tissue is destroyed and cannot be examined.
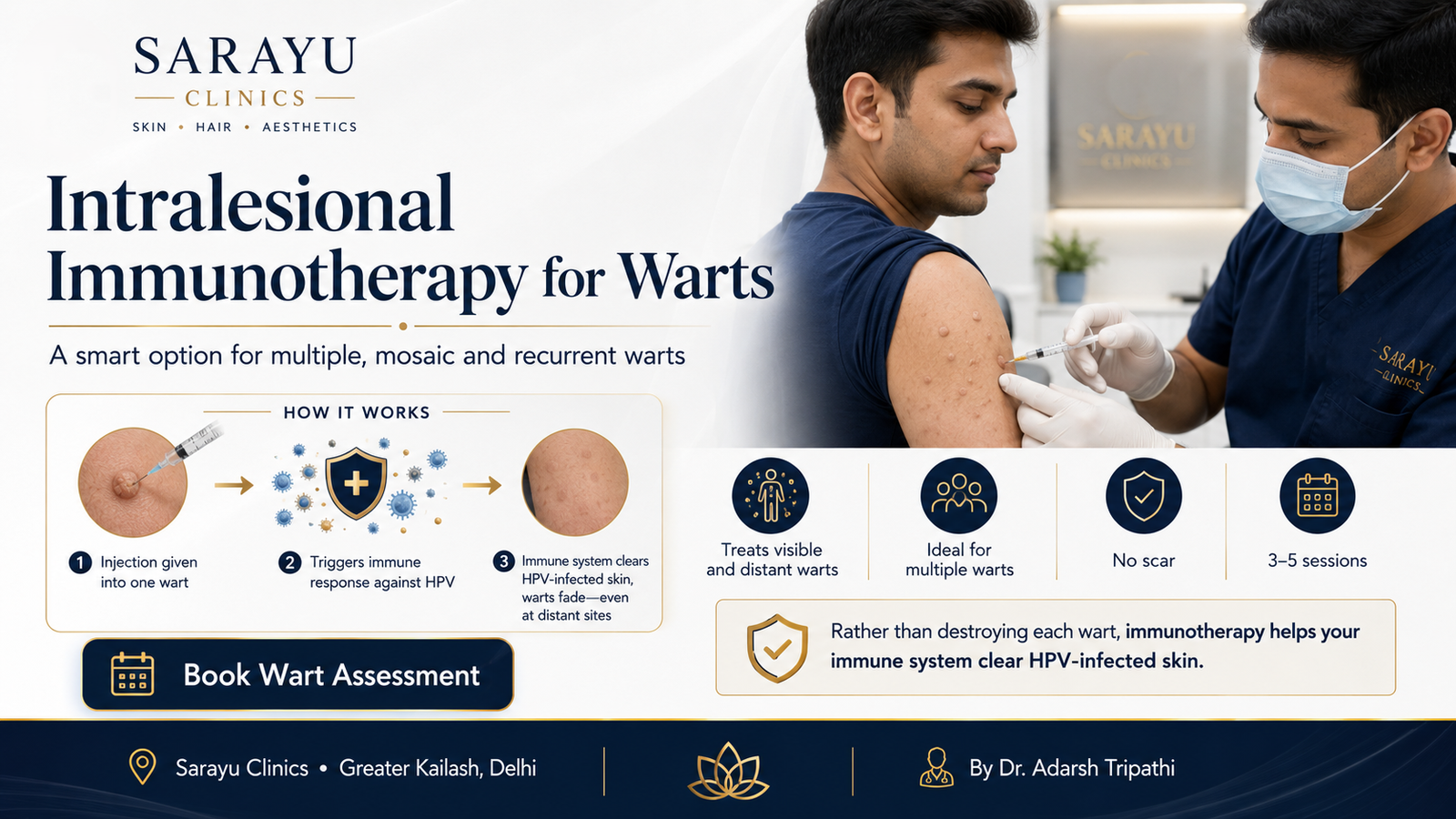
Intralesional immunotherapy — the one Delhi has largely ignored
Rather than destroying the wart, a small quantity of an antigen the immune system already recognises — most often autoclaved MMR vaccine, sometimes Candida antigen or PPD — is injected directly into it. The immune system arrives to deal with the antigen, encounters the HPV-infected cells sitting alongside it, and mounts a delayed-type hypersensitivity response against them.
The consequence is the interesting part. Warts elsewhere on the body — never injected, never touched — frequently clear at the same time, because the immune response is systemic rather than local. This is the only treatment on this page that addresses the reservoir of infected skin rather than the visible lump, and it is therefore the most rational choice for multiple warts, mosaic warts, recalcitrant warts and children with many lesions who would need dozens of freezing sessions otherwise.
It requires three to five sessions at two-to-three-week intervals. It works more slowly than a laser. It leaves no scar. It is not appropriate in pregnancy, in immunosuppression, or in anyone with a relevant vaccine allergy. And it is barely mentioned on any wart page in Delhi, despite being the treatment a dermatologist would want for their own recalcitrant warts.
Surgical excision — and why it is usually the wrong answer
It seems logical to cut a wart out. In practice it is a poor choice for most warts, for two reasons. The virus persists in the skin at the edges of the excision, so the wart frequently recurs — inside the scar, where it is harder to treat than it was before. And you now have a scar. Excision is reserved for lesions that need histopathology, for a small number of large or awkward warts, and for cases where a diagnosis is in doubt. It is not a routine wart treatment, whatever a clinic that has built a page around it may suggest.
Other agents, in specific hands
- Cantharidin — a blistering agent applied in clinic, painless on application, popular in paediatric practice.
- Intralesional bleomycin — effective for recalcitrant plantar and periungual warts. Painful. Restricted use.
- Topical 5-fluorouracil — particularly useful for flat warts on the face and in children.
- Imiquimod — an immune response modifier, principally used for anogenital warts.

Facial and Filiform Warts: Where a Surgeon Matters
On the back of a hand, a wart removal scar is a fact of life. On the eyelid margin, the vermilion border of the lip, or the rim of the nostril, it is the outcome. These are the sites where filiform warts most commonly appear, and they are precisely the sites where a facial plastic surgeon‘s training is not a marketing line.
- The eyelid margin. Cryotherapy here risks damage to the lash follicles and a permanent pale patch. Aggressive cautery risks notching the lid margin. Precise, superficial radiofrequency, with the globe protected, is the technique.
- The vermilion border. The line where lip meets skin is the most unforgiving landmark on the face. A millimetre of misalignment is visible across a room. Warts sitting on it are approached with a surgeon’s caution.
- The nasal ala and nostril rim. Over-treatment here produces notching and a visible contour deformity that is difficult to reconstruct.
- Flat warts across the face, especially after shaving. Dozens of small lesions. Aggressive ablation of each one, in Fitzpatrick IV–V skin, produces dozens of small pale or dark marks. This is a case for topical treatment or immunotherapy, not for a laser and an afternoon.
Where scarring is a concern, the principles are the same ones set out on our mole removal page: incisions along relaxed skin tension lines, layered closure, and — where a scar remains prominent at six to eight weeks — dermasanding to blend its edge.
Plantar Warts
Warts on the sole are pushed inward by body weight, which makes them deep, flat and genuinely painful — patients describe walking on a pebble. They are also, because of that depth, the most stubborn common wart to clear.
- Confirm it is a wart first. Use the skin-lines and black-dots test above. A great many people treating a plantar wart are treating a corn.
- Paring matters. The overlying callus must be pared down before any topical agent can reach the wart. This is done in clinic, not with a blade at home.
- Salicylic acid, with patience, remains first line. Daily, for months, with regular paring.
- Do not over-treat with heat or cold. A scar on the weight-bearing sole is permanently painful in a way the wart was not. This is the one site where the treatment can leave you worse off than the disease.
- Mosaic plantar warts are an immunotherapy problem. Freezing forty fused warts individually is neither kind nor effective.
- If you are diabetic, do not self-treat a lesion on your foot with an over-the-counter acid. See a doctor. This is not caution for its own sake.
Anogenital Warts: Honest Signposting
Sarayu Clinics is a facial plastic and aesthetic practice. We do not treat anogenital warts, and we would rather tell you where to go than take the booking.
What you should know. Anogenital warts are a sexually transmitted infection, caused predominantly by low-risk HPV types 6 and 11 — the same virus family, different strains. These strains cause visible warts but are not the ones associated with cancer. The high-risk types, chiefly 16 and 18, generally cause no visible lesion at all while carrying the risk of cervical, anal and oropharyngeal cancer. Having genital warts does not mean you have a cancer-causing strain, and having no warts does not mean you do not.
Anyone with anogenital warts should see a dermatologist, gynaecologist or genitourinary medicine specialist, should be offered screening for other sexually transmitted infections, should discuss partner notification, and — if female — should be up to date with cervical screening. Treatment options include imiquimod, podophyllotoxin, trichloroacetic acid, cryotherapy and surgical removal, and they belong in a service equipped to provide the rest of that care alongside.
A word on HPV vaccination
The vaccine prevents infection; it does not treat warts you already have. The current nonavalent vaccine covers types 6 and 11 — responsible for the large majority of anogenital warts — alongside the principal oncogenic types. An Indian-manufactured quadrivalent vaccine is also now available. Vaccination is most effective before exposure, which is why it is recommended in adolescence, but it remains worth discussing in adulthood. If you have recurrent warts, ask your doctor about it. It is the only intervention on this page that prevents rather than treats.
Benefits of Professional Wart Removal
- Correct diagnosis first. You find out whether it is a wart, a corn, a seborrhoeic keratosis or something that needs a biopsy — before anything is destroyed.
- Faster clearance than waiting. Especially for painful, spreading or long-standing lesions.
- Less spread. Treating warts promptly reduces autoinoculation to new sites and transmission to family members.
- Relief from pain. Plantar and periungual warts are genuinely disabling for some people.
- Minimal scarring in cosmetically critical sites. Eyelid, lip, nose — where technique determines the outcome.
- Immunotherapy clears warts you did not treat. For multiple lesions this is transformative, and it leaves no scar anywhere.
- Safety in diabetes and immunosuppression. Where self-treatment carries real risk of ulceration and infection.
Areas We Treat
- Face — flat warts, filiform warts around the eyelids, lips and nose
- Neck — filiform warts, often numerous
- Hands and fingers — common and periungual warts
- Around and under the nails
- Elbows and knees
- Soles of the feet — plantar and mosaic warts
- Scalp
- Trunk, arms and legs
Anogenital warts are not treated at this clinic. See the signposting section above.
Conditions & Concerns We Treat
- Common warts — single or few, on hands, knees and elbows.
- Plantar and mosaic warts — painful, deep, weight-bearing.
- Flat warts — multiple, facial, often spread by shaving.
- Filiform warts — cosmetically prominent, on eyelid, lip, nose and neck.
- Periungual warts — around the nail, distorting nail growth.
- Recalcitrant and recurrent warts — where previous destructive treatment has failed. This is an immunotherapy conversation.
- Warts in children — gentle protocols; often the right answer is topical treatment and patience rather than a frightening procedure.
- Skin tags, seborrhoeic keratoses and other lesions mistaken for warts — see mole and lesion removal.
- Atypical or non-responding lesions — assessed, and where indicated excised for histopathology rather than ablated.
The Procedure: Step by Step
- Assessment and diagnosis. Tripathi examines the lesion, confirms it is a wart, checks the skin lines and looks for thrombosed capillaries, and — where indicated — uses dermoscopy. Your immune status, diabetes, medications and pregnancy status are recorded, because all four change what is appropriate.
- A conversation about whether to treat at all. If you have one small, painless, non-spreading wart and a functioning immune system, we will tell you that watchful waiting is reasonable. If you would still rather have it gone, that is your decision to make with full information.
- Choosing the method. Number of warts, type, site, your skin type and how much scarring that site can tolerate. Multiple warts point toward immunotherapy; a single filiform wart on the lip points toward precise radiofrequency; a plantar wart points toward paring and salicylic acid before anything else.
- Local anaesthesia, where the method requires it. Radiofrequency, laser and excision are performed under local anaesthetic. Cryotherapy and immunotherapy usually are not, though topical numbing helps children.
- All visible warts are treated in the same session wherever practicable, because leaving one behind leaves a source. Depth is controlled deliberately — the endpoint is the wart, not the dermis beneath it.
- Specimen handling, where a lesion is atypical. If there is any doubt about the diagnosis, tissue is preserved and sent for histopathology. Destructive methods cannot do this, which is why the decision is made beforehand.
- Aftercare and the anti-spread conversation. Written instructions, and a frank discussion of the behaviours that reseed warts: picking, scratching, nail-biting, shaving over lesions, sharing towels and razors, and bare feet in changing rooms.
- At three to four weeks. Recurrence is discussed as an expectation to be managed, not a failure to be surprised by.
Downtime & Aftercare
- Cryotherapy: stinging during and for an hour after. A blister — sometimes a blood blister — forms within a day and dries over a week. Do not deroof it. Repeat sessions every two to three weeks.
- Radiofrequency or laser: a small crust that separates over seven to fourteen days. Keep it clean and covered. Do not pick it off.
- Immunotherapy: mild soreness and flu-like symptoms occasionally, for a day. No wound, no scar. The wart shrinks over weeks rather than disappearing on the day.
- Plantar warts: expect discomfort walking for a few days after any destructive treatment. Cushioned padding helps.
- SPF 50+ on any treated area of the face, for at least three months. UV on healing skin in Fitzpatrick IV–V produces post-inflammatory hyperpigmentation, which is a far more visible outcome than the wart was.
- Stop touching it. The single most useful thing you can do to prevent new warts is to stop picking at the ones you have. Cover them if you cannot resist.
- Do not share razors, towels, nail clippers or files, and do not shave over a wart. Wear sandals in communal showers and around pools.
Wart Removal Cost in Delhi
Warts are usually priced per lesion for destructive treatments and per session for immunotherapy. Verified Delhi ranges:
Treatment | Typical cost (INR)* |
Consultation & diagnosis | Rs 2,500 – Rs 5,000 |
Topical salicylic acid (prescription, per course) | Rs 200 – Rs 800 |
Cryotherapy — per wart, per session | Rs 500 – Rs 2,000 |
Cryotherapy — session for multiple warts | Rs 2,000 – Rs 6,000 |
Radiofrequency ablation / electrocautery — per wart | Rs 1,000 – Rs 5,000 |
CO2 laser — per wart | Rs 1,500 – Rs 8,000 |
Laser or RF — session for multiple warts | Rs 4,000 – Rs 15,000 |
Intralesional immunotherapy — per session | Rs 1,500 – Rs 4,000 |
Immunotherapy — full course of 3–5 sessions | Rs 5,000 – Rs 18,000 |
Filiform wart on eyelid, lip or nasal rim | Rs 2,000 – Rs 8,000, by site and complexity |
Excision with histopathology (atypical lesions) | Rs 5,000 – Rs 25,000, plus Rs 800 – Rs 2,500 for the laboratory |
*Indicative ranges only. Cryotherapy is cheap per session and typically needs three to six of them, so compare total course cost. For multiple warts, immunotherapy is frequently cheaper than freezing each lesion repeatedly — and it leaves no scars. Ask for the total, not the headline.
Prices shown are for guidance only. Your final treatment cost will be confirmed during the initial consultation, based on your individual needs, concerns, and personalised treatment plan.
Results Timeline
Timeframe | What usually happens |
Day 0 | Cryotherapy: stinging, then a blister. RF or laser: the wart is gone; a small crust remains. Immunotherapy: nothing visible. |
Week 1–2 | Crusts and blisters separate. New skin beneath is pink. Immunotherapy patients see nothing yet — this is normal. |
Week 3–4 | Review. Repeat cryotherapy if needed. Immunotherapy: the injected wart begins to shrink. |
Week 6–8 | Immunotherapy: distant, untreated warts begin regressing. This is the point at which patients become believers. |
Month 3 | Most destructive treatments complete. Pink marks fading. Course of immunotherapy finishing. |
Month 3–6 | Recurrences, where they occur, usually appear in this window. This is expected, and it is why we review. |
Month 6–12 | Post-treatment marks resolve. In Fitzpatrick IV–V skin, pigmentation may take the full twelve months to settle. |
Comparing Your Options
Treatment | Best for | Sessions | Scarring risk | Treats distant warts? | Biopsy possible? |
Salicylic acid | Common, plantar; compliant patients | Daily, 8–12 weeks | Very low | No | No |
Cryotherapy | Common, single or few | 3–6 | Low; pale marks possible | No | No |
Radiofrequency | Filiform, single common, periungual | 1–2 | Moderate if too deep | No | No |
CO2 laser | Periungual, plantar, awkward sites | 1–2 | Moderate if too deep | No | No |
Immunotherapy | Multiple, mosaic, recalcitrant | 3–5 | None | Yes | No |
Excision | Atypical or non-responding lesions | 1 | Certain — a scar | No | Yes |
Read the last two columns together. Only immunotherapy treats what you cannot see. Only excision tells you what it was. Everything else destroys a lump and hopes.
Are You a Good Candidate?
Treatment is clearly worthwhile if your wart:
- Is painful, or interferes with walking, writing or work
- Is spreading, or new ones keep appearing
- Is on the face, and bothers you
- Has been present for more than two years
- Is bleeding, changing, or has not responded to previous treatment
- Occurs alongside diabetes, immunosuppression, or pregnancy — where self-treatment is unwise
- Simply bothers you. A valid reason, honestly stated.
A different plan, or a delay, applies if you:
- Are pregnant — several agents, including immunotherapy and some topicals, are deferred
- Are immunosuppressed — warts are more numerous, more stubborn, and more likely to be atypical; assessment matters more, and immunotherapy may be inappropriate
- Are diabetic with a lesion on the foot — do not use over-the-counter acids; see a doctor
- Have a keloid tendency — destructive treatment on the trunk and shoulders needs care
- Have a lesion that is growing, bleeding, ulcerated, or is a solitary new warty lesion after the age of fifty — this needs a biopsy before it needs a laser
- Have anogenital warts — you need a service that can also offer STI screening and partner care. That is not this clinic, and we will refer you
Why Choose Sarayu Clinics for Wart Removal in Delhi ?
Warts are easy to burn off and easy to get wrong. At Sarayu Clinics they are assessed and treated by facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi, alongside co-founder Dr. Nidhi Bhatia.
- Diagnosis before destruction. Skin lines, thrombosed capillaries, dermoscopy where indicated. We establish what the lesion is before we make it impossible to find out.
- We will tell you when not to treat. Many warts clear on their own. A small, painless, static wart on a healthy child may need six months rather than liquid nitrogen.
- Immunotherapy, offered properly. For multiple, mosaic or recalcitrant warts, treating the immune reservoir rather than each lump is the rational approach — and it clears warts we never touched, without a scar anywhere.
- Honest about recurrence. No treatment eradicates HPV. We say so before you pay, not after your wart returns.
- Surgical precision where the site demands it. Eyelid margin, vermilion border, nasal rim. These are not places for enthusiasm with a cautery pen.
- Histopathology when a lesion is atypical. A wart that will not respond gets a biopsy, not a fourth session. Destructive methods destroy the evidence.
- Honest scope. We do not treat anogenital warts. We will tell you exactly where to go instead.
Medical Review & Sources
This page is for general information and is medically reviewed by the team at Sarayu Clinics under Dr. Adarsh Tripathi. It is not a substitute for an in-person clinical assessment. A warty lesion that fails to respond to appropriate treatment, grows, bleeds or ulcerates should be assessed and biopsied rather than treated again. Anogenital warts are not treated at this clinic and require a service that can also provide sexual health screening. Sources:
How to Reach Us:
Phone: +91 9289111081 , +91 9289111082
Email: sarayuinquiries@gmail.com
Sarayu Clinics website: www.sarayuclinics.com
Facebook: https://www.facebook.com/sarayuclinic
Instagram: https://www.instagram.com/sarayuclinics/
Dr. Adarsh Tripathi’s profile: https://dradarshtripathi.com/
Online Booking: Visit our website https://sarayuclinics.com/contact-us/ to schedule appointments conveniently.
How much does wart removal cost in Delhi?
Cryotherapy runs roughly Rs 500 to Rs 2,000 per wart per session, and usually needs three to six sessions. Radiofrequency or electrocautery is Rs 1,000 to Rs 5,000 per wart; CO2 laser Rs 1,500 to Rs 8,000. Intralesional immunotherapy costs Rs 1,500 to Rs 4,000 per session over a course of three to five. Prescription salicylic acid costs a few hundred rupees. For multiple warts, immunotherapy is often cheaper overall than repeatedly freezing each lesion — and it leaves no scars.
Do warts come back after removal?
Often, and the reason matters. No treatment destroys human papillomavirus. Cryotherapy, laser, radiofrequency and surgery all destroy the visible wart, but the virus persists in the normal-looking skin around it. Whether it returns depends on your immune system, not on the machine. Single common warts recur relatively rarely; plantar, mosaic and multiple warts recur far more often, because the reservoir of infected skin is larger. Recurrence is expected biology rather than treatment failure — and any clinic promising permanent removal in one session is not describing the infection.
How do I know if it's a wart or a corn?
Look at the skin lines — the fine ridges on your sole or fingertip. A wart interrupts them: the lines stop at the edge and go around. A corn preserves them: the lines run straight across. A wart usually shows tiny black dots, which are clotted blood vessels, not seeds or roots. And warts hurt when squeezed from the sides, while corns hurt when pressed directly downward. This takes thirty seconds and it decides the treatment.
Will warts go away on their own?
Frequently, yes. A substantial proportion of common warts in people with healthy immune systems clear without any treatment within one to two years, as the immune system finally recognises the infected cells. This is why watchful waiting is a legitimate option for a small, painless, non-spreading wart — particularly in children. Treatment becomes clearly worthwhile when a wart is painful, spreading, on the face, long-standing, or when you are diabetic or immunosuppressed.
What is intralesional immunotherapy for warts?
An antigen your immune system already recognises — most often autoclaved MMR vaccine, sometimes Candida antigen or PPD — is injected into a single wart. The immune system responds to the antigen, notices the HPV-infected cells beside it, and mounts a response against them. The remarkable part is that warts elsewhere on the body, never injected, frequently clear at the same time, because the response is systemic. It takes three to five sessions, works more slowly than a laser, and leaves no scar anywhere. It is the most rational treatment for multiple, mosaic or recalcitrant warts, and it is barely offered in Delhi.
Is laser wart removal better than cryotherapy?
Not inherently. Laser and radiofrequency remove the wart in a single visit under local anaesthetic, which suits filiform warts and single lesions in awkward places. Cryotherapy is cheaper per session but needs three to six of them, and it provokes a helpful local immune response as a side effect. Neither destroys the virus, so recurrence rates are broadly comparable. For multiple warts, neither is the right answer — immunotherapy is.
Can a wart be cancer?
Rarely, but importantly, yes. Squamous cell carcinoma, verrucous carcinoma and amelanotic melanoma can all present as a rough, wart-like lesion that does not respond to treatment. Features that should prompt a biopsy rather than another session: a wart that has failed two or more appropriate treatments, one that is growing steadily, one that bleeds spontaneously, one that has become painful or ulcerated, or a solitary new warty lesion in an adult over fifty. Cryotherapy, laser and radiofrequency all destroy the tissue, so no specimen can be examined — which is why the decision to biopsy is made before treatment, not after.

Should I have a wart surgically excised?
Usually not. Cutting a wart out seems logical, but the virus persists in the skin at the edges of the excision, so the wart frequently recurs inside the scar — and you now have a scar as well. Surgical excision is reserved for lesions that need histopathological examination, for a small number of large or awkward warts, and where the diagnosis is uncertain. It is not a routine wart treatment.
Are warts contagious?
Yes. HPV spreads by direct skin contact, by contact with contaminated surfaces such as changing-room floors and shared towels, and by autoinoculation — scratching one wart and seeding another. It enters through microscopic breaks in the skin, which is why nail-biting produces periungual warts and shaving spreads flat warts across the face. Do not share razors, towels or nail clippers; wear sandals in communal showers; and stop picking.
Does the HPV vaccine treat warts I already have?
No. The vaccine prevents infection with the HPV types it covers; it does not clear an existing infection. The current nonavalent vaccine covers types 6 and 11, which cause the large majority of anogenital warts, along with the main cancer-causing types. It is most effective before exposure, which is why it is given in adolescence, but it remains worth discussing in adulthood — particularly if you have recurrent warts. It is the only intervention that prevents rather than treats.
{kind=link}
{kind=link}