Depigmentation Treatment in Delhi
Depigmentation Treatment in Delhi
This is a page about a single confusing word, and the confusion is worth clearing up before anything else, because the two things people mean by ‘depigmentation’ are opposites.
Most people who search for depigmentation treatment want less pigment in particular places — the dark patches of melasma, the marks acne leaves behind, the uneven tone from years of Delhi sun. They want an even complexion. That is not, strictly speaking, depigmentation at all. It is pigmentation reduction, and it is treatable, and most of this page is about it.
A much smaller number of people mean the precise clinical thing: the deliberate, permanent removal of the pigment that remains in someone with extensive vitiligo, so that a face which is already mostly white becomes uniformly so. That is real depigmentation. It uses a drug that destroys pigment cells, it cannot be undone, and it is a serious decision reserved for a narrow set of circumstances. We cover it honestly further down.
At Sarayu Clinics in Greater Kailash, both conversations are had with facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi. And there is a third thing some people mean, which we will not do at all, and which we explain — and decline — plainly.
The short answer : ‘Depigmentation’ means two opposite things. // ONE — reducing dark patches (what most people want): melasma, post-acne marks, sun spots and uneven tone are treated by suppressing excess melanin and gently exfoliating, using topicals, chemical peels, and pigment-targeting lasers. This restores EVEN tone; it does not make you lighter than your natural colour. // TWO — clinical depigmentation therapy (the dermatology meaning): the deliberate, permanent removal of remaining pigment using monobenzone (MBEH), reserved for people with vitiligo affecting more than 50 percent of the body who have chosen to even out toward white because repigmentation has not worked. It destroys melanocytes, it is irreversible, and it demands lifelong sun protection. // THREE — skin whitening for fairness: we do not offer this, and the section below explains why. // Everyday pigmentation reduction in Delhi costs roughly Rs 1,500-15,000 per session depending on method. Monobenzone therapy is a specialist, long-term, carefully-consented treatment. The first step for anyone is a correct diagnosis of which pigment problem they actually have.
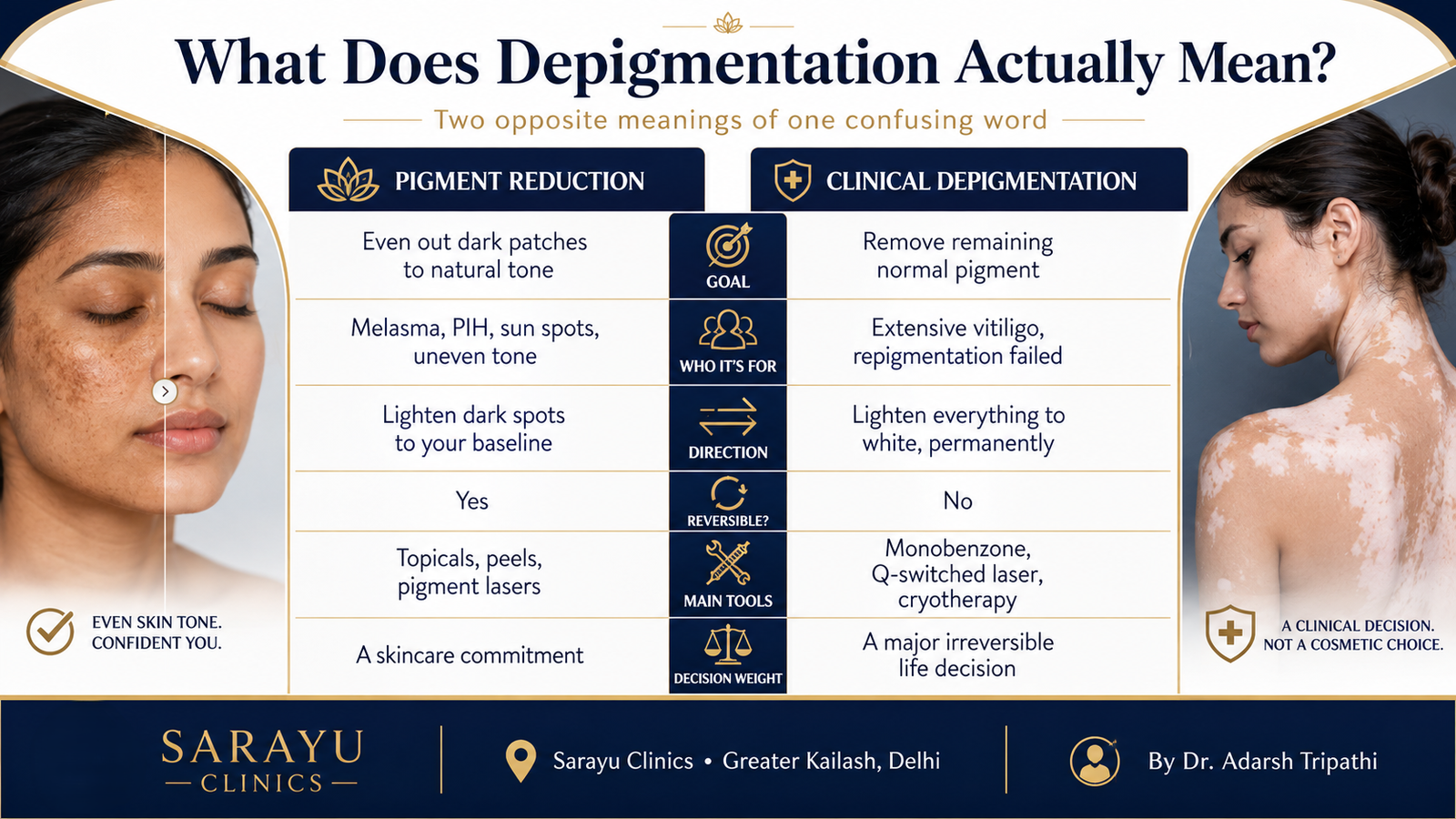
What Does Depigmentation Actually Mean?
Two people can type the same word and want opposite outcomes. Here is the distinction laid out plainly, because no other page in Delhi will do it for you.
| Pigmentation reduction | Clinical depigmentation therapy |
What you want | Fewer dark patches; even tone | Removal of remaining normal pigment |
The goal | Match dark areas back to your natural skin | Match residual pigment to large white patches |
Who it’s for | Melasma, PIH, sun spots, tanning | Extensive vitiligo (>50% body), repigmentation failed |
Direction | Lighten the dark spots to your baseline | Lighten everything to white, permanently |
Reversible? | Yes — it’s suppression and turnover | No — melanocytes are destroyed |
Main tools | Topicals, peels, pigment lasers | Monobenzone (MBEH), Q-switched lasers, cryotherapy |
How common | The large majority of searches | Rare, and a major life decision |
If you are in the left-hand column, read the next section. If you are in the right-hand column, skip to ‘Monobenzone and Vitiligo Depigmentation’ below. If you are not sure, that is exactly what a consultation is for.
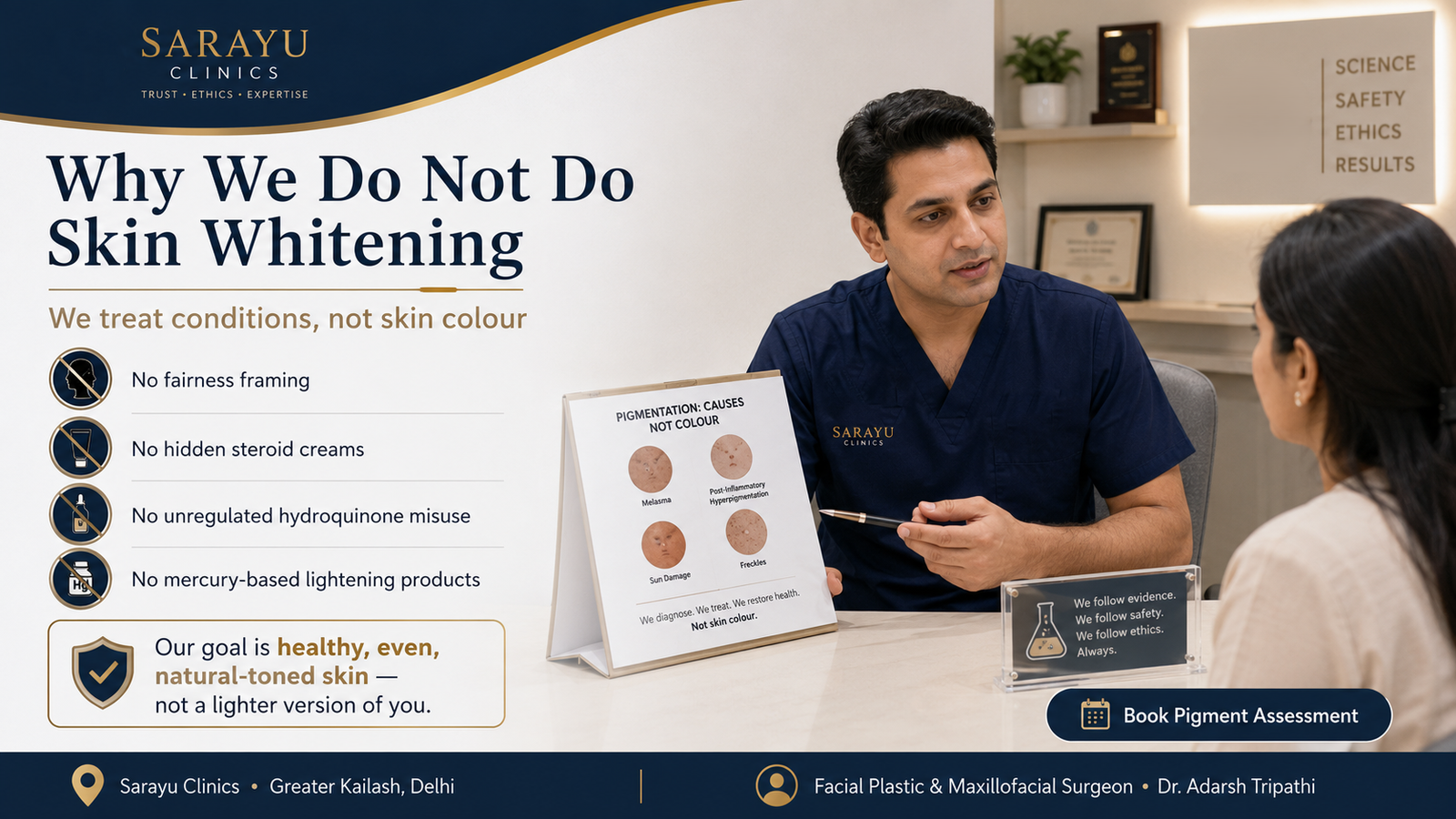
Why We Do Not Do Skin Whitening ?
There is a third thing ‘depigmentation’ is sometimes used to sell, and we want to be clear about it before we go any further: making healthy, evenly-toned brown skin permanently lighter than it naturally is, for the sole reason that lighter is considered more desirable.
We do not offer that, and we will not. Not because the chemistry is impossible — some of the same agents are involved — but because it is bad medicine and a worse idea. The products sold for it, particularly unregulated ones, cause real harm: exogenous ochronosis, a paradoxical blue-black darkening from long-term unsupervised hydroquinone; steroid damage from the corticosteroids hidden in many fairness creams; and mercury poisoning from illegal imports. And the premise itself — that your natural colour is a problem to be corrected — is one we do not accept and will not build a treatment around.
What we treat instead, and how we frame it : We treat conditions, and we restore evenness. If you have melasma, we treat the melasma. If acne has left dark marks, we treat the marks. If the sun has mottled your skin, we even it out. The goal in every case is to return your skin to its own healthy, uniform colour — not to move it along a scale toward pale. That distinction is not word-play. It changes which treatments are appropriate, which are safe, and what ‘success’ looks like. A good result is skin that looks like your skin, on a good day, evenly. It is not a lighter version of you.
Reducing Dark Patches (What Most People Want)
If you searched ‘depigmentation’ because you have dark spots, patches or uneven tone you would like reduced, this is your section — though the treatment is really pigmentation treatment, and our dedicated hub covers the full detail. The single most important thing is the same thing that decides everything in pigment: how deep the pigment sits.
Pigment in the upper layer of skin lifts relatively easily. Pigment that has dropped into the deeper layer is stubborn, responds slowly, and is easily made worse by aggressive treatment. Getting this wrong — treating deep pigment as though it were shallow — is how pigmentation is darkened rather than lightened, and it is the commonest mistake in the category.
The conditions behind ‘dark patches’
- Melasma — symmetrical brown or grey-brown patches, usually on the cheeks, forehead and upper lip. Hormonally driven, worsened by sun and heat, chronic. The one that most needs gentleness. See melasma treatment.
- Post-inflammatory hyperpigmentation (PIH) — the dark marks left behind by acne, injury or inflammation. Common in Indian skin because our melanocytes react strongly to inflammation. See acne marks versus acne scars.
- Sun-induced pigmentation and tanning — mottled tone, dark patches and lentigines from cumulative UV. A genuine and heavy factor in Delhi.
- Uneven tone and dullness — the general loss of clarity that pollution, sun and time produce.
- Periorbital pigmentation — dark circles of pigmentary rather than structural origin. See under-eye treatment.
How these are treated
The approach is layered, and it starts with the least aggressive option, because in Indian skin aggression provokes pigment. Topical agents that suppress melanin production and speed turnover; a course of gentle chemical peels using the right acid for your skin; and, where appropriate, pigment-targeting lasers such as Q-switched laser toning. Above all, rigorous daily sun protection, because none of the rest works without it. The full framework — depth diagnosis, the treatment menu, and the honest limits — is on the pigmentation treatment page.
The one rule that governs all of it : Pigment reduction in Indian skin is a marathon, not a procedure. Fast, aggressive treatment aimed at a quick result is precisely how post-inflammatory hyperpigmentation and rebound darkening are produced — the melanocyte responds to injury by making MORE pigment. Every credible pigment protocol in Fitzpatrick IV-V skin is gentle, gradual, sun-protected and patient. Anyone promising to clear your melasma in two sessions is describing a risk, not a result.
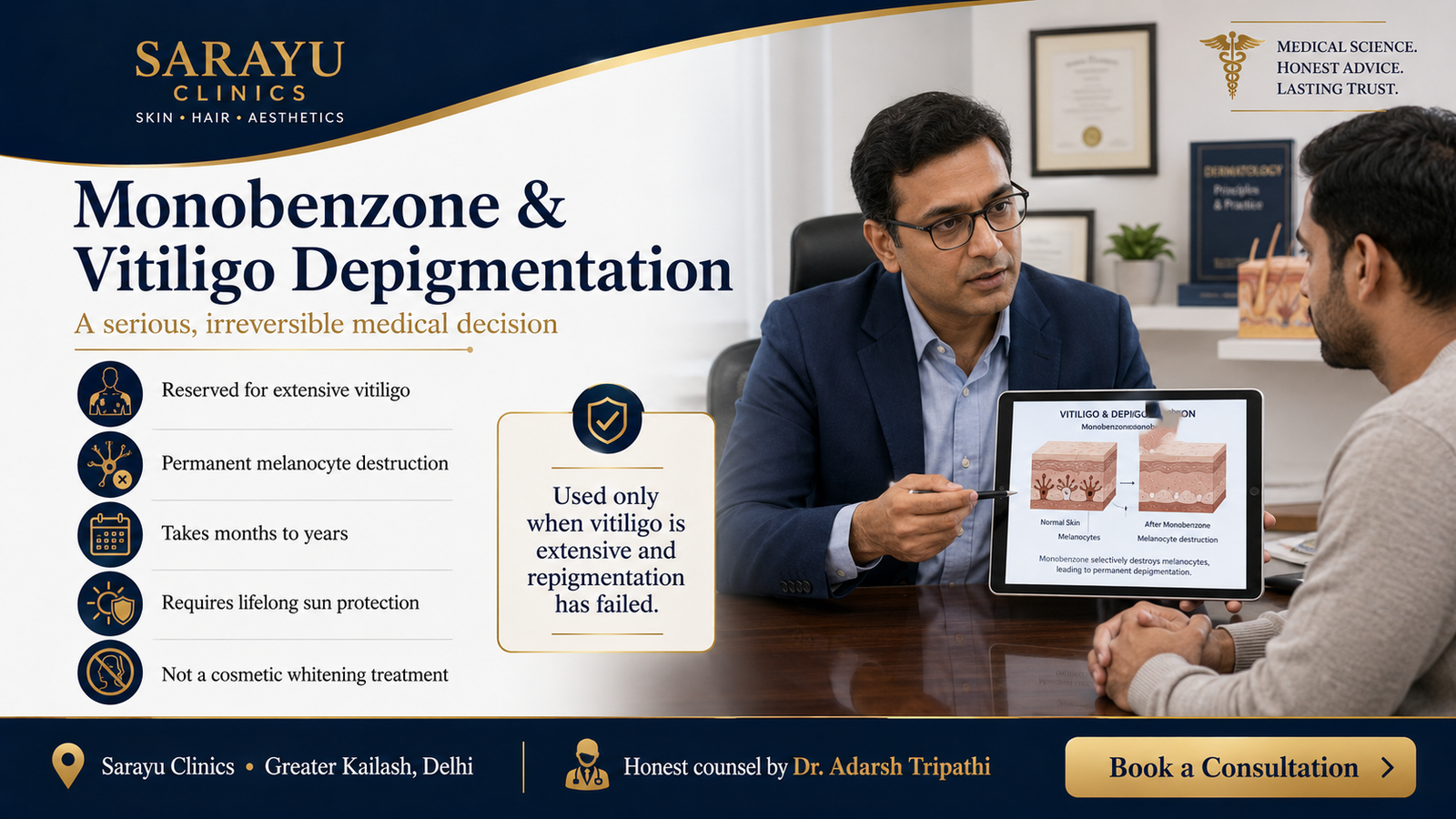
Monobenzone and Vitiligo Depigmentation (The Clinical Meaning)
Now the other meaning of the word — the true, technical one — handled with the seriousness it needs, because this is an irreversible medical decision and not a cosmetic treatment.
Vitiligo is an autoimmune condition in which the immune system destroys melanocytes, leaving white patches on normal-coloured skin. Most vitiligo is treated by trying to bring the colour back — with topical medicines, phototherapy, and sometimes surgical grafting. That is repigmentation, and it is the goal for the great majority of people with the condition.
Depigmentation therapy is the opposite strategy, and it is chosen in a specific and difficult situation: when vitiligo is extensive — generally more than half the body surface — when attempts to restore colour have failed, and when the daily distress of living with two colours has become greater than the prospect of becoming one uniform colour, even though that colour is white. In that situation, rather than fighting to repigment small remaining islands of normal skin, the remaining pigment is deliberately and permanently removed so that the whole skin matches.
What monobenzone is, and what it does
The agent is monobenzyl ether of hydroquinone — monobenzone, or MBEH. It is the only drug approved by the US FDA specifically for depigmentation in extensive vitiligo. Its history is instructive: it was discovered in the 1930s when rubber-factory workers wearing gloves treated with it developed permanent patches of pigment loss. It does not merely suppress melanin like a brightening cream — it generates free radicals that destroy the melanocytes themselves, permanently, in the skin it is applied to.
- It is permanent and irreversible. Once the melanocytes are gone, they are gone. There is no returning to your previous colour.
- It is slow. Depigmentation takes many months, sometimes one to two years, and requires touch-up sessions.
- It can be patchy, and it can repigment. Sun exposure can drive uneven return of pigment, which is one reason sun protection afterwards is absolute.
- It carries real risks. Local irritation and contact dermatitis are common; at high doses there are concerns around genetic and immune effects. It is a serious drug, not a cosmetic.
- It demands lifelong sun protection. Skin without melanin has lost its natural defence against ultraviolet radiation, raising the long-term risk of sun damage and skin cancer. SPF becomes a permanent, daily, non-negotiable part of life.
Physical methods — Q-switched ruby or alexandrite lasers, and cryotherapy — are sometimes used alongside or instead of monobenzone to remove residual pigment. The principle and the permanence are the same.
How this decision should be made : Depigmentation for vitiligo is one of the few genuinely irreversible decisions in aesthetic and dermatological medicine, and it should be made slowly. Before starting, a person should fully understand: that it is permanent; that it is slow and needs maintenance; that the result may be uneven and can partially reverse with sun exposure; that lifelong strict sun protection is required, both to hold the result and to guard against skin cancer; and that becoming uniformly white carries its own psychological, social and cultural weight that deserves to be talked through, with family and often with a mental health professional, before a drop of anything is applied. This is not a treatment anyone should be talked into, or sold. It is a considered choice, made by the patient, with time.
The medical management of vitiligo itself — the repigmentation side, with phototherapy and grafting — is a chronic-disease dermatology service, and where that is what you need, we will point you toward appropriate specialist care rather than pretend otherwise. Our role sits at the assessment, the surgical and the honest-counsel end of this conversation.
Benefits of Getting This Right
- A correct diagnosis first. Which of the two meanings applies to you, and which specific condition you actually have. Almost everything downstream depends on this and almost nobody starts here.
- Even tone, safely restored. For the everyday case, a gradual return to your own uniform colour, without the rebound darkening that aggressive treatment causes.
- No fairness framing, and no fairness products. No hidden steroids, no unregulated hydroquinone, no mercury. We treat conditions, not skin colour.
- Honest counsel on monobenzone. If clinical depigmentation is genuinely what you are considering, an honest account of its permanence and its weight — not a sale.
- Protection of the skin barrier and melanin where it belongs. Melanin is protective. We do not remove it casually, and we protect what remains.
- A surgeon’s judgement on the whole face. Pigment rarely travels alone; it comes with texture, laxity and structure, and is best assessed by someone who can see all of it.
Areas We Treat
- Face — cheeks, forehead, upper lip, chin (melasma, PIH, sun damage)
- Under-eyes — pigmentary dark circles
- Neck — poikiloderma, uneven tone, tanning
- Décolletage and chest
- Hands and forearms — sun pigmentation and lentigines
- Back, shoulders and arms — post-acne pigmentation
- For clinical vitiligo depigmentation, any affected area, assessed individually
Conditions & Concerns
- Melasma — the most common and the most delicate. See melasma treatment.
- Post-inflammatory hyperpigmentation — from acne, injury, or over-aggressive prior treatment.
- Sun spots, lentigines and tanning — cumulative UV damage.
- Uneven tone and dullness — the general case.
- Periorbital (under-eye) pigmentation — the pigmentary kind. See under-eye treatment.
- Extensive vitiligo, where depigmentation is being considered — assessed with the seriousness it deserves.
- Exogenous ochronosis — the paradoxical darkening caused by long-term unsupervised hydroquinone or fairness creams. We see this, and it needs the offending product stopped, not more of it.
A diagnostic note: pigment sitting flat in the skin is a pigmentation problem; a textural pit is a scar; a raised or changing spot may be something that needs a mole and lesion assessment. They are different problems with different treatments.
The Process: Step by Step
- Diagnosis, and which meaning applies. Tripathi establishes whether you want pigment reduced or pigment removed, and — for the everyday case — which condition you have and how deep the pigment sits. A Wood’s lamp or dermoscopy helps read the depth.
- A conversation about goals, and about fairness. We establish that the goal is even, healthy, natural-coloured skin. If what is being sought is fairness for its own sake, we say honestly that this is not something we treat, and why.
- For pigment reduction — priming and sun protection first. A topical protocol and rigorous SPF are begun before any procedure, because they reduce the risk of the treatment itself causing pigmentation.
- For pigment reduction — the graded plan. Topicals, then gentle peels, then pigment-targeting laser only where indicated — escalating slowly, watching how your skin responds at each step.
- For clinical depigmentation — extended informed consent. A different process entirely: a full discussion of permanence, timeline, maintenance, sun-protection obligations and the psychosocial weight, with time and, where helpful, family and psychological input, before anything begins.
- Treatment, at the right pace. Slow and monitored in both cases, for opposite reasons — one to avoid provoking pigment, the other because the drug itself works slowly and irreversibly.
- Review and long-term protection. Regular review, and lifelong sun protection — protective for pigment reduction, essential for depigmentation.
Downtime & Aftercare
- Topical pigment treatment: no downtime; possible mild irritation and purging as the routine beds in. Results are gradual, over weeks to months.
- Chemical peels: mild flaking for a few days in the superficial case. See the chemical peel page for detail.
- Pigment lasers (toning): little to no downtime; a course is needed, spaced out, and over-treatment risks worsening pigment.
- Monobenzone therapy: irritation and contact dermatitis are common; the depigmentation itself unfolds over many months. The commitment is measured in years, not visits.
- SPF 50+ every single morning, indefinitely. For pigment reduction, sunscreen IS the treatment — without it nothing holds. For depigmentation, it is a lifelong medical necessity, because skin without melanin cannot defend itself against UV.
- Stop any fairness cream, steroid cream or unregulated lightening product under supervision. Several of these are actively causing the problem they claim to fix.
The Procedure: Step by Step
- Skin assessment and honest suitability check. Tripathi assesses hydration, texture, skin quality and the specific area of concern. If your dominant problem is volume, sagging, pigment or scarring, SkinVive is the wrong treatment and you will hear that before you book it.
- Allergy screening. Specifically for lidocaine allergy, previous allergic reaction to hyaluronic acid fillers, a history of anaphylaxis or multiple severe allergies, and allergy to Gram-positive bacterial proteins. All four are contraindications.
- Product verification. Ask to see the sealed Allergan syringe, its batch number and packaging — whether it is labelled SkinVive or Juvéderm Volite. We will show you before it is opened.
- Topical anaesthetic is applied, though SkinVive contains 0.3% lidocaine itself, which does much of the work. This is the most comfortable of the skin-quality injectables.
- Microdroplet injection. An ultrafine 32-gauge needle deposits many small droplets across the cheek, spaced roughly five millimetres to a centimetre apart, so the gel distributes evenly. A typical session uses two to three millilitres and takes well under an hour.
- Immediate aftercare. Small bumps and mild redness are expected and settle within hours. A cool compress, and written instructions before you leave.
- Optional touch-up at one month. Assessed at review rather than assumed. Some patients need it; many do not.
- Every six to nine months to sustain the result.
Downtime & Aftercare
- First few hours: small bumps at the injection points and mild redness. These are the most common effects and they settle quickly — this is the lowest-downtime injectable in the skin-quality category.
- Possible for 1–4 weeks: mild swelling, small lumps, bruising, tenderness. Uncommon, usually minor, and self-resolving. Reported in the clinical data and worth knowing about.
- First 24 hours: avoid strenuous exercise, extensive sun or heat exposure, saunas, steam and alcohol.
- Do not book laser, chemical peel or other procedures immediately afterwards without telling your doctor. There is a possible risk of an inflammatory reaction at the treatment site. This is in the manufacturer’s own safety information and it is routinely ignored.
- Delay treatment if you have skin sores, pimples, rashes, hives, cysts or infection in the area.
- SPF 50+ daily. Standard, and non-negotiable.
- Return to work: the same day, in almost every case.
Cost in Delhi
The two meanings occupy different worlds, financially as well as clinically. Verified Delhi ranges:
Treatment | Typical cost (INR)* |
Consultation, diagnosis & Wood’s lamp assessment | Rs 2,500 – Rs 5,000 |
Topical pigment-reduction protocol (per month) | Rs 1,500 – Rs 5,000 |
Chemical peel course — pigment (per session) | Rs 1,500 – Rs 8,000 |
Q-switched laser toning (per session) | Rs 3,000 – Rs 10,000 |
Laser toning — course of 6+ | Package pricing after assessment |
Combination pigment plan (topicals + peels + laser) | Individualised after assessment |
Vitiligo depigmentation — monobenzone (per month) | Rs 3,000 – Rs 8,000, over many months |
Q-switched laser / cryotherapy for residual pigment | Assessed and quoted individually |
Skin whitening for fairness | Not offered. See the section above. |
*Indicative ranges only. Pigment reduction is a course, not a session, so compare on total plan cost and on realistic timelines rather than a headline price. Monobenzone therapy is a multi-year commitment and should be costed as one.
Prices shown are for guidance only. Your final treatment cost will be confirmed during the initial consultation, based on your individual needs, concerns, and personalised treatment plan.
Counterfeits and the two-name problem
Allergan products are heavily counterfeited worldwide, and the SkinVive/Volite dual naming creates an additional opening for confusion. Ask to see the sealed syringe, the batch number, the outer packaging and, if relevant, the import documentation — whichever name is on the box. A price substantially below the ranges above is a warning rather than a saving. Any clinic that becomes uncomfortable when asked these questions has already answered them.
Results Timeline
Timeframe | Pigment reduction | Monobenzone depigmentation |
Weeks 1–4 | Skin settles into the topical routine; possible mild irritation. No dramatic change yet. | Irritation begins. No visible depigmentation yet. |
Month 2–3 | First honest lightening of superficial pigment. Melasma responds slowly. | Gradual patchy lightening starting in treated areas. |
Month 3–6 | Clear, photographable evening of tone with a consistent regimen. | Depigmentation spreading and deepening. Uneven at this stage. |
Month 6–12 | Near the realistic endpoint for most everyday pigment. Maintenance begins. | Approaching uniform depigmentation. Touch-ups continue. |
Beyond 12 months | Ongoing maintenance and sun protection hold the result. | Result maintained with lifelong sun protection; repigmentation guarded against. |
Both are slow. Neither is a quick fix, and any promise of one is a warning sign — in the everyday case because speed causes rebound pigment, and in the clinical case because the drug simply does not work quickly.
Pigment Reduction vs Depigmentation, Side by Side
| Pigment reduction | Monobenzone depigmentation |
Purpose | Even out dark patches to natural tone | Remove all remaining pigment, permanently |
Reversible | Yes | No |
Who it suits | Melasma, PIH, sun damage, uneven tone | Extensive vitiligo, repigmentation failed |
Mechanism | Suppress melanin, exfoliate, target pigment | Destroy melanocytes |
Timeline | Weeks to months | One to two years, then maintenance |
Sun protection | Protective; makes treatment work | A lifelong medical necessity |
Main risk | Rebound pigment if over-treated | Permanence; skin cancer risk from lost melanin |
Decision weight | A skincare commitment | A major, irreversible life decision |
What We Will Not Do ?
- We will not make healthy skin lighter than its natural colour for fairness. Explained above, and meant.
- We will not prescribe unsupervised long-term hydroquinone. It causes exogenous ochronosis — a paradoxical, stubborn darkening — when used without breaks and monitoring.
- We will not treat pigment aggressively for a fast result. In Indian skin that manufactures the rebound pigmentation it claims to treat.
- We will not sell monobenzone as a cosmetic. It is an irreversible medical decision for a narrow indication, not a lightening treatment.
- We will not treat a pigmented lesion that should be examined. A changing or atypical spot is assessed, not bleached.
Why Choose Sarayu Clinics ?
This is a page on which we have spent as many words on what we will not do as on what we will. That is the practice. Pigment is assessed and treated at Sarayu Clinics by facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi, alongside co-founder and celebrity aesthetician Dr. Nidhi Bhatia.
- We tell you which ‘depigmentation’ you actually want. Reduction or removal — opposite treatments, and the confusion is resolved before anything is prescribed.
- We treat conditions, not skin colour. Even, healthy, natural tone is the goal. Fairness is not a treatment we offer.
- Gentle, graded, sun-protected pigment protocols. Because Indian skin punishes aggression with rebound pigment.
- Honest counsel on monobenzone. If clinical depigmentation is genuinely your situation, the permanence and weight of it, in full — with time to decide.
- We recognise the damage fairness products cause. Ochronosis, steroid damage, mercury. We stop them; we do not add to them.
- A surgeon’s read of the whole face. Pigment travels with texture, laxity and structure. It is best judged by someone who sees all of it.
Medical Review & Sources
This page is for general information and is medically reviewed by the team at Sarayu Clinics under Dr. Adarsh Tripathi. It is not a substitute for an in-person clinical assessment. Monobenzone depigmentation is an irreversible medical treatment reserved for extensive vitiligo and requires thorough informed consent and lifelong sun protection. This clinic does not provide skin-whitening or fairness treatment. Sources:
How to Reach Us:
Phone: +91 9289111081 , +91 9289111082
Email: sarayuinquiries@gmail.com
Sarayu Clinics website: www.sarayuclinics.com
Facebook: https://www.facebook.com/sarayuclinic
Instagram: https://www.instagram.com/sarayuclinics/
Dr. Adarsh Tripathi’s profile: https://dradarshtripathi.com/
Online Booking: Visit our website https://sarayuclinics.com/contact-us/ to schedule appointments conveniently.
What does 'depigmentation' actually mean?
It has two opposite meanings. In everyday use, most people mean reducing dark patches — melasma, acne marks, sun spots — to restore an even tone. That is really pigmentation reduction. In clinical dermatology, depigmentation means the deliberate, permanent removal of the pigment that remains in someone with extensive vitiligo, using a drug that destroys pigment cells, so that a mostly-white face becomes uniformly white. The two are opposites, and the first step is establishing which one you want.
How much does depigmentation treatment cost in Delhi?
For everyday pigment reduction: topical protocols run Rs 1,500-5,000 a month, pigment chemical peels Rs 1,500-8,000 per session, and Q-switched laser toning Rs 3,000-10,000 per session, usually as a course. For clinical vitiligo depigmentation with monobenzone, the cost is roughly Rs 3,000-8,000 a month over many months to a couple of years. Because both are courses rather than single treatments, judge them on total plan cost and realistic timelines.
Is depigmentation permanent?
It depends which meaning applies. Pigment reduction for melasma, acne marks or sun damage is not permanent — it suppresses excess melanin and speeds turnover, and it needs maintenance and sun protection to hold. Clinical depigmentation with monobenzone IS permanent and irreversible: it destroys the melanocytes, and there is no returning to your previous colour. That permanence is exactly why it is reserved for extensive vitiligo and decided slowly.
What is monobenzone, and is it safe?
Monobenzone (monobenzyl ether of hydroquinone, MBEH) is the only drug FDA-approved for depigmentation in extensive vitiligo. Unlike a brightening cream, it does not suppress melanin — it destroys the cells that make it, permanently. It is appropriate only in specific circumstances: vitiligo affecting more than half the body, where attempts to restore colour have failed. It causes irritation and contact dermatitis commonly, carries concerns at high doses, and commits the person to lifelong strict sun protection because skin without melanin cannot defend itself against UV. It is a serious medical treatment, not a cosmetic, and it should never be used to lighten normal skin.
Can you make my skin fairer or whiter?
No. We do not offer skin whitening or fairness treatment, and we do not accept the premise that natural brown skin is a problem to be corrected. What we do treat is uneven tone and specific pigment conditions — melasma, post-acne marks, sun damage — with the goal of returning your skin to its own even, healthy, natural colour. Beyond the ethics, the products sold for fairness cause real harm: exogenous ochronosis from unregulated hydroquinone, damage from hidden steroids, and mercury poisoning from illegal creams.
Why is my pigmentation getting darker with treatment?
Two common reasons. First, over-aggressive treatment: in Indian skin, melanocytes respond to injury by producing more pigment, so a harsh peel or laser aimed at a quick result can darken pigmentation rather than lighten it. Second, exogenous ochronosis: long-term unsupervised use of hydroquinone or fairness creams causes a paradoxical blue-black darkening that is stubborn and distressing. If your pigment is worsening with treatment, the treatment is very likely the cause, and the answer is to stop and reassess, not to intensify.
What's the difference between this and pigmentation treatment?
For the everyday meaning, there is no real difference — reducing dark patches IS pigmentation treatment, and our pigmentation page covers the full detail of depth diagnosis and the treatment menu. This page exists mainly to clear up the confusing word ‘depigmentation’, which also has a second, opposite, clinical meaning that pigmentation pages do not address: the deliberate removal of remaining pigment in extensive vitiligo.

Can depigmentation treat my melasma?
If by depigmentation you mean reducing the dark patches, yes — melasma is treated by suppressing excess melanin with topicals, gentle chemical peels and careful laser toning, always slowly and with rigorous sun protection. But melasma is chronic and hormonally driven, it responds slowly, and it is easily worsened by aggressive treatment, so expectations matter. What you do NOT want for melasma is the clinical, monobenzone sense of depigmentation, which is for vitiligo and is entirely inappropriate here.
Is laser depigmentation safe for Indian skin?
Pigment-targeting laser toning can be safe and useful in Indian skin, but only in careful hands and at conservative settings, because the same melanin that lasers target is also what makes darker skin prone to post-inflammatory hyperpigmentation. Over-treatment is a real risk and can worsen pigment. This is why laser is layered in after topicals and peels, as part of a graded plan, rather than reached for first — and why it should be done by someone who treats Indian skin regularly.
Should I consider depigmentation for my vitiligo?
Only in specific circumstances, and only after careful thought. Depigmentation is considered when vitiligo is extensive — generally more than half the body — and when treatments to restore colour have not worked, and when living with two colours has become more distressing than the prospect of becoming uniformly white. It is permanent and irreversible, it takes a year or more, it demands lifelong sun protection, and becoming uniformly white carries real psychological and social weight. It should be discussed thoroughly, with family and often a mental health professional, and never rushed or sold. For most people with vitiligo, the goal is repigmentation, not depigmentation.
{kind=link}
{kind=link}