Dermabrasion in Delhi
Dermabrasion in Delhi
Two treatments share most of a name and almost nothing else. One is a gentle exfoliating facial that takes twenty minutes, costs a couple of thousand rupees and leaves you looking slightly brighter by evening. The other is a surgical procedure performed under anaesthesia, in which a high-speed rotating burr abrades the skin down into the dermis until it bleeds, and from which you recover over several weeks.
The first is microdermabrasion. The second is dermabrasion. They are separated by a factor of several hundred in the depth of tissue removed. Almost everyone who types ‘dermabrasion’ into a search engine means the first one, and a fair number of clinic websites are content to let that confusion stand, because the surgical word lends weight to the cosmetic treatment.
We would rather be precise. At Sarayu Clinics in Greater Kailash, this page is written by facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi, and it will tell you three things. What microdermabrasion actually does, and does not do. Why we do not perform full-face dermabrasion on Indian skin, and what the evidence says about why nobody else should either. And where dermabrasion genuinely still earns its place — in a surgeon’s hands, on a scar, several weeks after an excision.

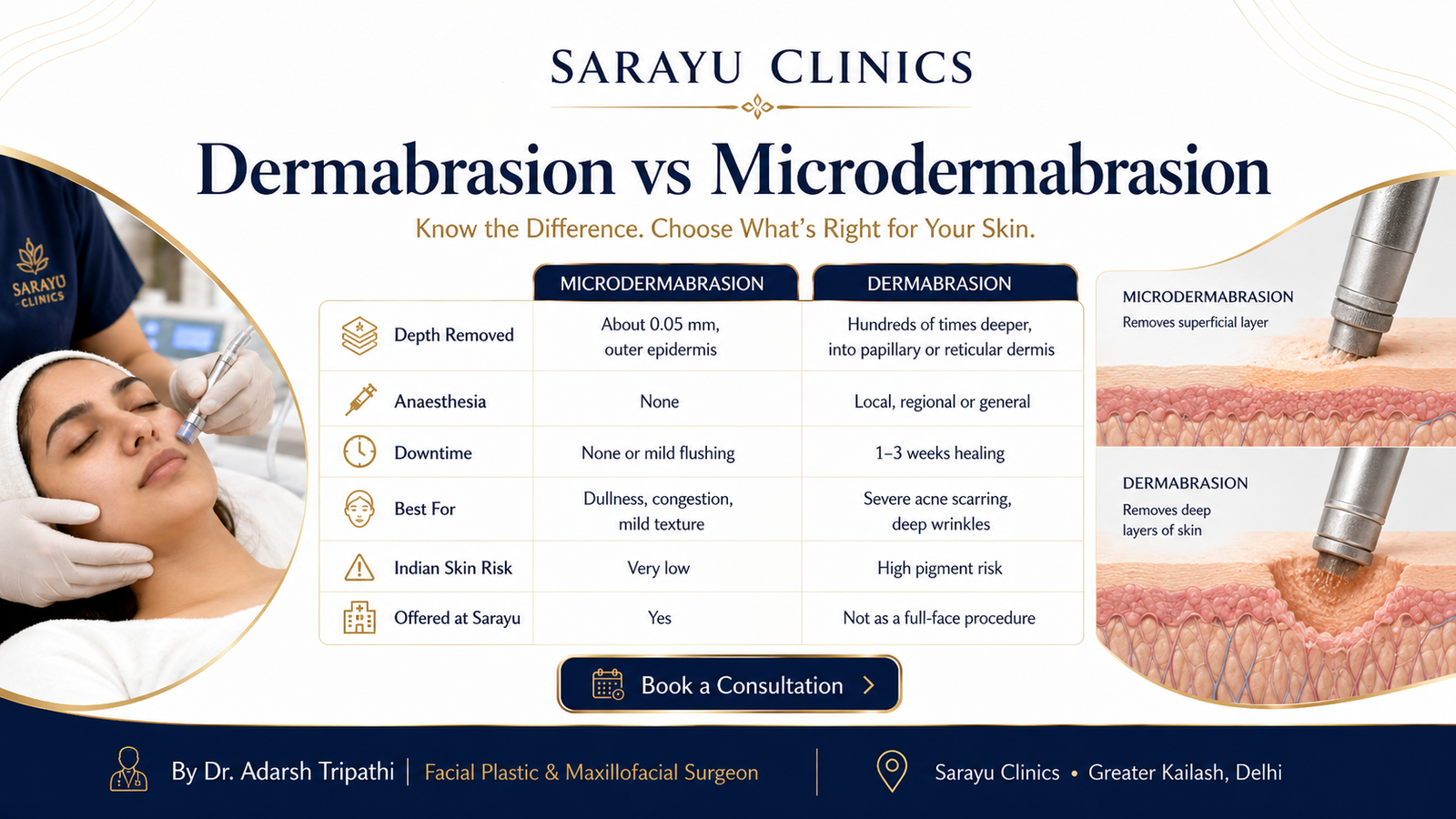
The short answer : MICRODERMABRASION removes roughly 0.05mm of skin — the dead outer layer of the epidermis — using a crystal spray or a diamond-tipped wand. No anaesthesia, no downtime, mild results, safe in every skin type. Good for dullness, congestion and texture; useless for scars, wrinkles and deep pigment. Delhi cost Rs 1,500–5,000 per session. // DERMABRASION removes hundreds of times more, reaching the papillary or reticular dermis, using a motorised wire brush or diamond fraise under anaesthesia. It was the standard treatment for severe acne scarring and deep wrinkles until ablative lasers superseded it in the 1990s. It is safest in Fitzpatrick I–II skin. From type IV upward — most Indian patients — it can cause dyspigmentation that is permanent. We do not perform it as a full-face resurfacing procedure. // DERMASANDING, or manual spot dermabrasion, is the exception: a surgeon-performed technique used to blend a surgical scar at six to eight weeks after excision. It has good evidence behind it and it remains a legitimate part of facial plastic surgery. That is where dermabrasion still belongs.
Dermabrasion vs Microdermabrasion
If you read nothing else on this page, read this table. The names are similar. The procedures are not.
| Microdermabrasion | Dermabrasion |
Depth removed | About 0.05mm — the outer epidermis | Hundreds of times deeper — full epidermis into the papillary or reticular dermis |
Instrument | Crystal spray or diamond-tipped wand | Motorised wire brush or diamond fraise |
Anaesthesia | None | Local, regional or general anaesthesia |
Setting | Treatment room | Operating theatre, in the classical form |
Bleeding | None | Yes — pinpoint dermal bleeding is the surgical endpoint |
Downtime | None. Mild flushing for an hour | 1–3 weeks of healing; weeks to months of redness |
Treats | Dullness, congestion, mild texture | Severe acne scarring, deep wrinkles, rhinophyma, tattoos (historically) |
Risk in Indian skin | Very low | High — potentially permanent pigment loss and demarcation lines |
Sessions | A course of 6–10 | One, and rarely repeated |
Offered at Sarayu? | Yes | Not as a full-face procedure. See dermasanding below |
A clinic advertising ‘dermabrasion’ at a facial price, with no downtime and no anaesthetic, is offering you microdermabrasion. That is fine — it is a perfectly good treatment — but you should know which one you are buying, because the two answer entirely different questions.

Why We Do Not Perform Full-Face Dermabrasion ?
Dermabrasion was, for three decades, the best thing medicine had for severe acne scarring and deeply etched wrinkles. Surgeons of an earlier generation performed it with skill and courage, and patients with fair skin got results that nothing else could deliver. It is not a bad procedure. It is a procedure that has been overtaken, and one that was never well suited to the skin most of our patients have.
The evidence on skin tone is not ambiguous
Dermabrasion works by removing the full thickness of the epidermis, which is where your melanocytes live. When the skin re-epithelialises, pigment cells repopulate it unevenly. In pale skin the result is usually acceptable. In darker skin it is not.
The clinical literature is consistent and blunt about this. Dermabrasion is safest in Fitzpatrick skin types I and II. From type III upward, the risk of post-operative hyperpigmentation and hypopigmentation rises. In Fitzpatrick type IV and above — which describes the great majority of Indian patients — dermabrasion can cause significant dyspigmentation that may be permanent. Not a temporary darkening that fades over eighteen months. Permanent loss of skin colour, often with a visible demarcation line where the treated area meets untreated skin at the jaw.
And better tools arrived thirty years ago
When ablative carbon dioxide and erbium lasers reached clinical use in the 1990s, dermabrasion was gradually retired for facial resurfacing. Lasers offered comparable results with markedly less hypopigmentation, less scarring and shorter recovery — because energy delivery can be controlled to a precision that a spinning burr against living skin simply cannot match. Fractional delivery, which spares columns of untreated skin between treatment zones, improved that safety margin again.
What we offer instead : If your concern is significant acne scarring, deep texture or photodamage, the modern answers in Indian skin are fractional resurfacing at conservative settings, radiofrequency microneedling, subcision and TCA CROSS for specific scar types, or — where the problem is structural rather than superficial — surgery. Each of these is staged, controllable and reversible in the sense that it does not permanently remove your natural skin colour. // If a clinic in Delhi has offered you full-face dermabrasion, ask them three questions. What is my Fitzpatrick type, and what is the published hypopigmentation risk at that type? Where will this be performed, and under what anaesthesia? Why is this a better choice for me than fractional laser? The quality of the answers will tell you a great deal. // A footnote that is rarely mentioned and matters to the people doing the work: dermabrasion aerosolises blood. It is one of the few aesthetic procedures with a genuine bloodborne exposure risk to the operator and the theatre staff, and it requires full protective equipment. That is not a reason to avoid it as a patient. It is a reason to be sceptical of anyone performing it casually.

Where Dermabrasion Still Wins: Dermasanding and Scar Revision ?
Having spent several hundred words explaining why we do not do the big version, here is the honest counterweight. There is one setting in which dermabrasion remains not merely acceptable but genuinely excellent, supported by controlled evidence, and difficult to replicate with anything else. It happens to be a facial plastic surgeon’s procedure rather than a dermatologist’s.
Blending a surgical scar
When a lesion is excised from the face — a mole, a cyst, a skin cancer — the resulting scar heals as a fine line. In most cases that is the end of it. But sometimes the scar sits slightly proud of the surrounding skin, or its edges catch the light, or its texture differs enough from the skin around it to draw the eye. At around six to eight weeks after the excision, when the scar is still remodelling, manual dermabrasion — dermasanding — of that small, specific area levels the scar edge with the surrounding skin and blends the transition. A prospective, randomised, blinded study supports its effect on the appearance of surgical scars.
This is not full-face resurfacing. It is a few square centimetres, treated with a hand-held abrasive under local anaesthesia, in a patient whose scar the surgeon created and whose healing he has been following. It is a direct downstream service of mole and lesion excision, and it is one of the reasons excision on the face is better done by someone who will still be looking after the scar two months later.
Perioral wrinkles, and the technique called laserbrasion
The deep vertical lines above the upper lip are among the hardest features on the face to treat. Skin there is thin and mobile, and filler often looks wrong. Combining CO2 laser resurfacing with manual dermasanding — a technique reported as laserbrasion — reduced heavy perioral wrinkles by around 95 per cent, compared with roughly 75 per cent for laser alone, with faster healing and, importantly, no significant long-term hypopigmentation in the reported series.
The caveat remains the caveat. That evidence comes from populations rather lighter than most of ours, and the periorbital and perioral skin of a Fitzpatrick V patient is not the skin those figures describe. We use this technique selectively, on carefully chosen patients, after a test area — traditionally behind the ear — has demonstrated how that individual’s skin responds. Where the answer is unclear, we do not proceed.
Rhinophyma and other specific indications
Dermabrasion also retains a role in reshaping rhinophyma — the thickened, bulbous nasal skin of advanced rosacea — and occasionally in contouring specific raised lesions. These are reconstructive rather than cosmetic uses, and they sit naturally within the practice of a facial plastic surgeon.
Microdermabrasion in Delhi
Now the treatment most people actually came here for. Microdermabrasion is a mechanical exfoliation of the outermost epidermis — roughly the thickness of a sheet of cling film — using either a spray of fine aluminium oxide crystals or, more commonly now, a diamond-tipped wand under gentle suction. Nothing is anaesthetised. Nothing bleeds. You may be slightly pink for an hour.
What it does well:
- Immediate brightness and smoothness. Removing the dead outer layer improves how light reflects off the skin. The effect is real and it is visible the same day.
- Congestion and blackheads. The suction extracts debris from the follicle opening.
- Better absorption of everything applied afterwards. Serums penetrate more effectively through a freshly exfoliated stratum corneum, which is why microdermabrasion is often paired with a mask or infusion.
- Very superficial texture and dullness. Sun-dulled, rough, tired-looking skin responds.
- Safety across every skin type. Because the epidermis is barely disturbed, the post-inflammatory hyperpigmentation risk in Fitzpatrick IV–V skin is minimal.
What it does not do, whatever it says on the brochure:
- It does not treat acne scars. Scars are dermal. Microdermabrasion never reaches the dermis. Not once, not over ten sessions.
- It does not treat wrinkles. For the same reason.
- It does not clear melasma or deep pigmentation. It lifts a little surface pigment. Dermal pigment is untouched, and vigorous microdermabrasion on melasma-prone skin can provoke it.
- It does not shrink pores permanently. It clears them, which makes them look smaller for a while.
A course of six to ten sessions at two-to-three-week intervals gives a cumulative improvement in skin quality. If your goals are more ambitious than that, a chemical peel course, microneedling or a HydraFacial will serve you better, and we will say so rather than sell you ten sessions of something that cannot reach your problem.
Benefits
Of microdermabrasion
- Same-day brightness — skin reflects light differently within hours.
- No downtime whatsoever — mild flushing that settles within an hour. Makeup the same day.
- Safe in every Fitzpatrick type — minimal pigmentation risk, which is not true of most resurfacing.
- Clears congestion and blackheads — suction extraction of the follicle opening.
- Affordable and repeatable — a sensible maintenance treatment rather than a transformation.
- Excellent preparation for other treatments — improves topical absorption for weeks.
Of surgical dermasanding, in its proper place
- Blends a surgical scar into surrounding skin — levels the edge and improves the light-catching texture difference that makes a scar visible.
- Supported by controlled evidence — a prospective, randomised, blinded study on surgical scar appearance.
- Precise and small — treats a few square centimetres, not a face. Risk scales with area.
- Stimulates collagen reorganisation — injury to the papillary dermis triggers new collagen and reorientation of existing fibres, which is part of how the scar improves.
- Performed by the surgeon who made the incision — continuity of care that a resurfacing clinic cannot offer.
Areas We Treat
Microdermabrasion:
- Full face
- Neck and décolletage
- Back and shoulders (for congestion and post-acne roughness)
- Backs of the hands
Dermasanding and spot dermabrasion:
- Individual surgical scars anywhere on the face
- Scars following mole, cyst or lesion excision
- Perioral rhytides (selected patients, after test patch)
- Rhinophyma and thickened nasal skin
- Traumatic scars and tattoo fragments embedded in a wound
Conditions & Concerns
- Dullness, roughness and congestion — microdermabrasion, in a course.
- Blackheads and clogged follicles — microdermabrasion, and see open pores treatment for the underlying cause.
- Surgical scars that catch the light — dermasanding at six to eight weeks, by the surgeon.
- Acne scarring — NOT microdermabrasion. See acne scar treatment for subcision, TCA CROSS, Morpheus8 and fractional CO2.
- Pigmentation and melasma — NOT dermabrasion, at any depth. See pigmentation treatment.
- Deep wrinkles — fractional resurfacing or RF microneedling. See MNRF.
One diagnostic point before you book anything for post-acne skin: flat dark patches are pigment, and pits are scars. They need entirely different treatments and neither responds to microdermabrasion. The acne marks versus acne scars guide gives you the thirty-second test.
The Procedure: Step by Step
Microdermabrasion
- Skin type, concern and expectations. If your goal is scars, wrinkles or melasma, we will tell you that this is the wrong treatment before you book a course of it.
- Cleansing and degreasing. Uneven surface oil produces uneven abrasion.
- A diamond-tipped wand under gentle suction, or a controlled crystal spray, passed systematically across the treatment area. Sensation is a mild scratching and pulling. It takes 20 to 30 minutes.
- Suction clears loosened debris from follicle openings.
- Infusion and finish. A serum, a mask or a hydrating step, then sunscreen. The freshly exfoliated skin absorbs it unusually well.
- The course. Six to ten sessions at two-to-three-week intervals, then maintenance.
Dermasanding for scar revision
- Excision first, and then patience. The lesion is removed and closed. Nothing is abraded for six to eight weeks while the scar remodels.
- Assessment at six weeks. Is the scar level? Is the texture matched? Many scars need nothing further, and we will say so.
- Test patch, where skin type demands it. Classically behind the ear, reviewed before proceeding on the face.
- Local anaesthesia. The small area is fully numbed.
- Manual abrasion. A hand-held abrasive levels the scar edge with the surrounding skin. The endpoint is judged visually, by depth and by pinpoint bleeding, and it is judged by the person who made the incision.
- Dressing, antiviral cover and aftercare. Herpes simplex reactivation is a recognised risk of dermabrasion; antiviral prophylaxis is standard where there is any history of cold sores.
- Review at two and six weeks. Sun protection is absolute during this window.
Downtime & Aftercare
- Microdermabrasion: mild pinkness and a slight tightness for an hour or two. Makeup the same day. Avoid retinoids, acids and scrubs for 48 hours. SPF 50+ the following morning.
- Dermasanding, a small area: a raw, weeping surface for three to five days, then a crust that separates over a week. Redness at the site persists for several weeks and fades over months. Keep it moist, keep it covered, do not pick.
- Sun protection is not aftercare. It is the treatment. SPF 50+ daily for a minimum of three months on any dermabraded area. UV on healing dermis in Indian skin is precisely how post-inflammatory hyperpigmentation is manufactured.
- Antiviral prophylaxis before any dermabrasion if you have ever had a cold sore. Reactivation across a raw dermis is a serious complication.
- Tell us before you book if you have taken isotretinoin. The conventional standard is a full year off isotretinoin before dermabrasion — twice the interval required before a chemical peel — because the skin’s healing behaviour is altered and scarring risk rises. More recent work suggests manual and microdermabrasion may be safer in this context than the classical motorised procedure, but this remains a conversation to have, individually, before anything is done.
- Active acne is a relative contraindication to dermabrasion, because mechanical abrasion across inflamed skin can spread bacteria and raise infection risk. Settle the acne first — see acne treatment.
Cost in Delhi
Verified Delhi ranges. Note that the two procedures on this page occupy entirely different price brackets, for entirely different reasons.
Treatment | Typical cost (INR)* |
Consultation & skin assessment | Rs 2,500 – Rs 5,000 |
Crystal microdermabrasion, per session | Rs 1,500 – Rs 4,000 |
Diamond-tip microdermabrasion, per session | Rs 2,000 – Rs 5,000 |
Microdermabrasion with serum infusion / mask | Rs 3,000 – Rs 7,000 |
Course of 6 microdermabrasion sessions | Package pricing — usually more economical |
Microdermabrasion, neck or hands (add-on) | Rs 1,000 – Rs 3,000 |
Dermasanding / spot dermabrasion of a scar | Rs 8,000 – Rs 25,000, by size and complexity |
Dermasanding combined with scar excision | Quoted as a surgical package after assessment |
Full-face classical dermabrasion | Not offered. See the section above. |
*Indicative ranges only. If a clinic quotes you ‘dermabrasion’ at Rs 2,000 with no downtime, they are quoting microdermabrasion. That is not dishonest pricing, but it is imprecise language, and you are entitled to ask which procedure you have actually booked.
Prices shown are for guidance only. Your final treatment cost will be confirmed during the initial consultation, based on your individual needs, concerns, and personalised treatment plan.
Results Timeline
Timeframe | Microdermabrasion | Dermasanding (scar) |
Day 0 | Mild pinkness. Skin already brighter and smoother to the touch. | Raw, weeping surface. Local anaesthetic wearing off. |
Day 3–7 | Effect at its best. Slight return of dullness by the end of the week. | Crust forms and separates. New epithelium beneath. |
Week 2–4 | Second session. Improvement is cumulative rather than dramatic. | Pink, flat, new skin. Scar looks worse before it looks better. |
Month 2–3 | After 4–6 sessions, a genuine, sustained improvement in texture and clarity. | Redness fading. Texture beginning to match surrounding skin. |
Month 6 | Maintenance every 4–6 weeks holds the result. | Near-final appearance. Blending assessed properly at this point. |
Month 12 | — | Full scar maturation. This is when a scar is judged, not before. |
Nobody should judge a scar before a year has passed. Scars look their worst at around six weeks — pink, firm, raised — and then improve steadily for twelve months. Half the scar revisions requested in Delhi are requested at week eight, on scars that would have settled on their own.
How These Compare to the Alternatives ?
Treatment | Depth reached | Best for | Indian skin safety | Downtime | Cost/session |
Microdermabrasion | ~0.05mm, epidermis | Dullness, congestion, texture | Excellent | None | Rs 1,500–5,000 |
Superficial chemical peel | Epidermis | Acne, epidermal pigment, texture | Excellent | 0–5 days | Rs 1,500–6,000 |
Microneedling | Papillary dermis, fractionally | Texture, early scars, collagen | Excellent | 1–2 days | Rs 5,000–10,000 |
RF microneedling | Dermis, with heat | Scars, laxity, deep texture | Excellent | 2–5 days | Rs 10,000–45,000 |
Fractional CO2 | Dermis, fractionally | Significant scarring, deep texture | Caution — real PIH risk | 5–10 days | Rs 8,000–20,000 |
Full-face dermabrasion | Papillary/reticular dermis, entirely | Historically: severe scars, deep wrinkles | High risk — permanent dyspigmentation | 2–3 weeks | Not offered |
Read the depth column, then read the safety column. That relationship is the whole of resurfacing. The reason fractional technologies replaced dermabrasion is not that they go deeper — several go shallower — but that they leave untreated skin between treated columns, from which the epidermis and its pigment cells repopulate evenly. Dermabrasion removes everything, everywhere, at once. In Indian skin, that difference is the difference between a good result and a permanent one.
Are You a Good Candidate?
Microdermabrasion suits you if you have:
- Dull, rough, congested skin with realistic expectations
- Blackheads and clogged follicles
- Any Fitzpatrick type — including IV, V and VI
- No downtime available and a modest budget
- A willingness to commit to a course rather than a single session
Dermasanding may be appropriate if you have:
- A surgical or traumatic facial scar that has been maturing for at least six to eight weeks
- A scar whose texture, rather than colour, is the problem
- A skin type that has demonstrated, on a test patch, that it will tolerate the abrasion
Neither procedure is appropriate, or a delay is needed, if you:
- Have taken isotretinoin — a full year off is the conventional standard before dermabrasion; discuss individually
- Have active, inflamed acne in the area — abrasion can spread bacteria and raise infection risk
- Have any history of cold sores — antiviral prophylaxis is required before dermabrasion
- Have a keloid or hypertrophic scarring tendency
- Have active rosacea, prominent broken capillaries or very thin skin in the area
- Have melasma — mechanical abrasion can provoke it
- Are using an unprescribed steroid or fairness cream — supervised withdrawal first
- Are pregnant or breastfeeding, for the surgical procedure
- Want acne scars, wrinkles or deep pigment treated by microdermabrasion — it cannot reach them, and we will not sell you a course pretending otherwise
Are You a Good Candidate for SkinVive?
You are likely well-suited if you:
- Are 21 or older with dull, dehydrated or rough-textured cheek skin
- Want improved skin quality with no change whatsoever to your facial shape
- Prefer a single session over a multi-session course
- Want the most comfortable of the skin-quality injectables
- Are vegetarian, Jain, or will not accept animal-derived products
- Have any Fitzpatrick skin type, I through VI
- Have reasonable expectations — improvement in good skin, not transformation of damaged skin
SkinVive is not for you, or needs careful discussion, if you:
- Have a history of anaphylaxis, or of multiple severe allergies
- Are allergic to lidocaine
- Are allergic to Gram-positive bacterial proteins
- Have had a previous allergic reaction to any hyaluronic acid filler
- Have a history of excessive or thick scarring — safety has not been studied and additional scarring may result
- Are taking therapy that suppresses the immune response — increased infection risk
- Are pregnant or breastfeeding — safety has not been studied
- Have skin sores, pimples, rashes, hives, cysts or infection in the treatment area — treatment should be delayed
- Are planning laser treatment or a chemical peel soon afterwards — tell your doctor; there is a risk of inflammatory reaction
- Want volume, lift, pigment correction or scar treatment — this is the wrong category entirely
Why Choose Sarayu Clinics ?
This is a page on which we have declined a procedure, corrected a widespread confusion, and told you that the cheaper treatment cannot do what the brochures claim. That is the practice. At Sarayu Clinics, resurfacing and scar revision are assessed and performed by facial plastic and maxillofacial surgeon Dr. Adarsh Tripathi, alongside co-founder and celebrity aesthetician Dr. Nidhi Bhatia.
- We tell you which procedure you are buying. Microdermabrasion is not dermabrasion, and we will not let the word do work it has not earned.
- We do not perform full-face dermabrasion on Indian skin. The published hypopigmentation risk from Fitzpatrick IV upward is not a risk we are willing to take with your face, and better tools have existed for thirty years.
- Scar revision by the surgeon who made the incision. Dermasanding at six to eight weeks post-excision is a facial plastic surgery technique, performed with continuity of care that a resurfacing clinic cannot offer.
- Test patches, antiviral cover, isotretinoin history. The unglamorous safety steps, taken every time, on every patient.
- Honest limits on microdermabrasion. It will not touch your acne scars. We would rather send you to the right treatment than sell you ten sessions of the wrong one.
- An honest ‘wait’. Half the scars we are asked to revise at week eight would have settled on their own by month twelve. We will tell you when to do nothing.
Medical Review & Sources
This page is for general information and is medically reviewed by the team at Sarayu Clinics under Dr. Adarsh Tripathi. It is not a substitute for an in-person clinical assessment. Full-face dermabrasion carries a substantial risk of permanent pigmentary change in Fitzpatrick skin types IV and above and is not performed at this clinic. Dermasanding for scar revision is undertaken selectively, after assessment and where appropriate a test patch. Sources:
How to Reach Us:
Phone: +91 9289111081 , +91 9289111082
Email: sarayuinquiries@gmail.com
Sarayu Clinics website: www.sarayuclinics.com
Facebook: https://www.facebook.com/sarayuclinic
Instagram: https://www.instagram.com/sarayuclinics/
Dr. Adarsh Tripathi’s profile: https://dradarshtripathi.com/
Online Booking: Visit our website https://sarayuclinics.com/contact-us/ to schedule appointments conveniently.
What is the difference between dermabrasion and microdermabrasion?
They are different procedures separated by hundreds of times in depth. Microdermabrasion removes roughly 0.05mm — the dead outer layer of the epidermis — with a diamond wand or crystal spray, needs no anaesthetic and has no downtime. Dermabrasion removes the full epidermis and reaches into the papillary or reticular dermis using a motorised wire brush or diamond fraise, under anaesthesia, with bleeding as the surgical endpoint and one to three weeks of healing. A clinic offering ‘dermabrasion’ at a facial price with no downtime is offering microdermabrasion.
How much does microdermabrasion cost in Delhi?
Crystal microdermabrasion runs Rs 1,500 to Rs 4,000 per session; diamond-tip Rs 2,000 to Rs 5,000; with a serum infusion or mask, Rs 3,000 to Rs 7,000. Because it works cumulatively, a course of six to ten sessions is the realistic commitment, and package pricing is usually more economical. Spot dermasanding of a surgical scar is a different procedure entirely, at Rs 8,000 to Rs 25,000 depending on size and complexity.
Is dermabrasion safe for Indian skin?
Full-face dermabrasion is not a treatment we recommend for most Indian patients. The clinical literature is consistent: dermabrasion is safest in Fitzpatrick skin types I and II, risk of pigmentary change rises from type III upward, and in type IV and above it can cause dyspigmentation that may be permanent — including loss of skin colour and a visible demarcation line at the jaw. Fractional lasers and radiofrequency microneedling achieve comparable results in Indian skin with far lower pigment risk. Microdermabrasion, by contrast, is safe in every skin type.
Will microdermabrasion get rid of my acne scars?
No. Acne scars are dermal — they sit below the layer microdermabrasion reaches, and no number of sessions will change that. Any clinic selling you a microdermabrasion course for scarring is selling you something that physically cannot work. Effective options are subcision for rolling scars, TCA CROSS for ice-pick scars, RF microneedling such as Morpheus8 or MNRF, and fractional CO2 laser — usually in combination. First establish that you have scars rather than flat dark marks, which are pigmentation and need a different treatment entirely.
Why did dermabrasion fall out of use?
Ablative carbon dioxide and erbium lasers arrived in the 1990s and delivered comparable or better resurfacing results with substantially less hypopigmentation, less scarring and shorter recovery. Energy delivery can be controlled with a precision that a rotating burr against living skin cannot approach, and fractional delivery — sparing columns of untreated skin between treatment zones — improved that safety margin again. Dermabrasion was gradually retired for facial resurfacing and survives now in specific, targeted indications.
What is dermasanding?
Manual dermabrasion of a small, specific area — usually a surgical scar — using a hand-held abrasive rather than a motorised burr. Performed around six to eight weeks after an excision, while the scar is still remodelling, it levels the scar edge with the surrounding skin and blends the textural transition that makes a scar catch the light. A prospective, randomised, blinded study supports its effect on surgical scar appearance. It is a facial plastic surgery technique, best performed by the surgeon who made the incision and has been following the healing.
Can dermabrasion treat wrinkles around the mouth?
It can, and the evidence is interesting. Combining CO2 laser resurfacing with manual dermasanding — a technique described as laserbrasion — reduced heavy perioral wrinkles by around 95 per cent, against roughly 75 per cent for laser alone, with faster healing and no significant long-term hypopigmentation in the reported series. The caveat is that those results come from lighter skin than most of our patients have. We use the technique selectively, in carefully chosen patients, after a test patch behind the ear has shown how that individual’s skin responds.

How long do I need to be off isotretinoin before dermabrasion?
The conventional standard is a full year — twice the interval usually required before a chemical peel — because isotretinoin alters how skin heals and raises the risk of abnormal scarring. More recent work suggests manual dermabrasion and microdermabrasion may be safer than the classical motorised procedure in patients with recent isotretinoin use, but this is a case-by-case discussion to have with your surgeon before anything is done, not a rule to assume.
Does microdermabrasion hurt?
No. Most people describe a mild scratching and a pulling sensation from the suction, comparable to a cat’s tongue. No anaesthetic is needed. Dermasanding, by contrast, is performed under local anaesthesia because it reaches the dermis, and the treated area is genuinely raw for several days afterwards.
How many microdermabrasion sessions will I need?
Six to ten, at two-to-three-week intervals, with maintenance every four to six weeks afterwards. It works cumulatively — a single session brightens the skin for about a week, but sustained improvement in texture and clarity comes from the course. If your goals are more ambitious than skin brightness and clearer follicles, a chemical peel course or microneedling will reach further and may prove better value.
{kind=link}
{kind=link}